

This is the second article in a series on heartburn and GERD. If you haven’t read the first one, I’d suggest doing that first.
The idea that heartburn is caused by too much stomach acid is still popular in the media and the public. But as Daniel pointed out in the comments section of the last post, anyone familiar with the scientific literature could tell you that heartburn and GERD are not considered to be diseases of excess stomach acid.
Instead, the prevailing scientific theory is that GERD is caused by a dysfunction of the muscular valve (sphincter) that separates the lower end of the esophagus and the stomach. This is known as the lower esophageal valve, or LES. The LES normally opens wide to permit swallowed food and liquids to pass easily into the stomach. Except for belching, this is the only time the LES should open.
Here’s the key point. It doesn’t matter how much acid there is in the stomach. Even a small amount can cause serious damage. Unlike the stomach, the lining of the esophagus has no protection against acid.
Free eBook
Learn More about Heartburn and GERD
Download this free eBook to discover the little-known causes of heartburn and GERD, and find out how to get rid of the problem forever.
"*" indicates required fields
I hate spam, too. Your email is safe with me. By signing up, you agree to our privacy policy.
We’ve Been Asking the Wrong Question
In an editorial published in the journal Gastroenterology, the author remarked: (1)
Treating gastroesophageal reflux disease with profound acid inhibition will never be ideal because acid secretion is not the primary underlying defect.
I couldn’t agree more. For decades the medical establishment has been directing its attention at how to reduce stomach acid secretion in people suffering from heartburn and GERD, even though it’s well-known that these conditions are not caused by excess stomach acid. Instead, the question researchers should have been asking is, “what is causing the LES to malfunction?” Since it is universally agreed upon that this is the underlying mechanism producing the symptoms of GERD, wouldn’t it make sense to focus our efforts here? That’s exactly what we’re going to do in this article.
GERD Is Caused by Increased Intra-Abdominal Pressure
It is well accepted in the literature that GERD is caused by an increase in intra-abdominal pressure (IAP).
For example, several studies have indicated an association between obesity and GERD, and one paper in Gastroenterology concluded that increased intra-abdominal pressure was the causative mechanism. (2, 3) But while I agree that all of the currently accepted factors play a role, I do not think they are the primary causes of the increased IAP seen in GERD.
The Two Primary Causes of Increased Intra-Abdominal Pressure
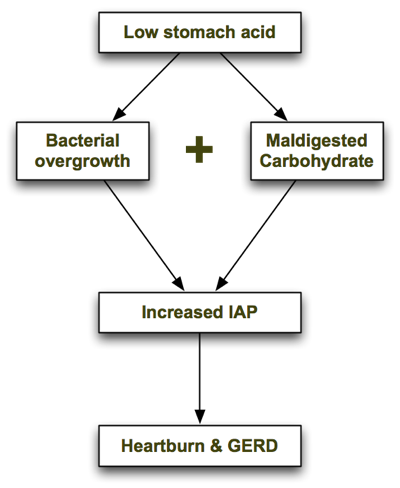
In his excellent book, Heartburn Cured, microbiologist Dr. Norm Robillard argues that carbohydrate malabsorption leads to bacterial overgrowth, resulting in IAP which drives reflux. Dr. Robillard makes a strong case that carbohydrate malabsorption plays a significant role in IAP, and I agree. But as I researched this issue I couldn’t help asking: what might be causing the carbohydrate malabsorption in the first place, and are there any other causes of bacterial overgrowth that may precede carbohydrate malabsorption? I believe the one answer to both of those questions is low stomach acid. Low stomach acid can contribute to both bacterial overgrowth (independently of carbohydrate intake) and carbohydrate malabsorption, as I describe below. In a nutshell, the process looks like this: Let’s look at each step in turn.
1. Low Stomach Acid Causes Bacterial Overgrowth
As I explain in the next article, one of the chief roles of stomach acid is to inhibit bacterial overgrowth. At a pH of 3 or less (the normal pH of the stomach), most bacteria can’t survive for more than 15 minutes. But when stomach acid is insufficient and the pH of the stomach rises above 5, bacteria begin to thrive. The gastrin knockout mouse, which is incapable of producing stomach acid, suffers from bacterial overgrowth—as well as inflammation, damage and precancerous polyps in its intestines. (4) It is also well documented that acid-suppressing drugs promote bacterial overgrowth. Long-term use of Prilosec, one of the most potent acid suppressing drugs, reduces the secretion of hydrochloric acid (HCL) in the stomach to near zero. In one trial, 30 people with GERD were treated with a high dose of Prilosec (40g/day) for at least 3 months. (5) Eleven of the 30 Prilosec-treated people had developed significant bacterial overgrowth, compared with only one of the 10 people in the control group.
2. Low Stomach Acid Causes Maldigestion of Carbohydrates
Stomach acid (HCL) supports the digestion and absorption of carbohydrates by stimulating the release of pancreatic enzymes into the small intestine. If the pH of the stomach is too high (due to insufficient stomach acid), the pancreatic enzymes will not be secreted and the carbohydrates will not be broken down properly.
Like what you’re reading? Get my free newsletter, recipes, eBooks, product recommendations, and more!
Bacterial Overgrowth + Maldigested Carbohydrates = GAS!
In Hearburn Cured, Dr. Robillard points out that though microbes are able to metabolize proteins and even fats, their preferred energy source is carbohydrate. The fermentation of carbohydrates that haven’t been digested properly produces gas. The resulting gas increases intra-abdominal pressure, which is the driving force behind acid reflux and GERD. From Dr. Robillard’s book:
According to Suarez and Levitt (17), 30 g of carbohydrate that escapes absorption in a day could produce more than 10,000 mL (ten liters) of hydrogen gas. That is a huge amount of gas!
When stomach acid is sufficient and carbohydrates are consumed in moderation, they are properly broken down into glucose and rapidly absorbed in the small intestine before they can be fermented by microbes. However, if stomach acid is insufficient and/or carbohydrates are consumed in excess, some of the carbs will escape absorption and become available for intestinal microbes to ferment.
Other Supporting Evidence
Dr. Robillard also argues that if gas produced by microbial fermentation of carbohydrates causes acid reflux, we might expect that reflux could be treated by either:
- Reducing bacterial overgrowth, or
- Reducing carbohydrate intake.
He points to two studies which demonstrate this. In a study by Pehl, administration of erythromycin (an antibiotic) significantly decreased esophageal reflux. (6)
In another study by Pennathur, erythromycin strengthened the defective lower esophageal sphincter in patients with acid reflux. (7) To my knowledge, there have only been two small trials performed to test the effects of carbohydrate restriction on GERD. Both had positive results. A small case series showed a significant, almost immediate resolution of GERD symptoms in obese individuals initiating a very-low-carb diet. (8) A more recent study found that a very low-carb diet decreased distal esophagus acid exposure and improved the symptoms of GERD. (9) Perhaps most importantly, the magnitude of the improvement was similar to what has been reported with treatment with proton-pump inhibitors (acid suppressing drugs).
Some researchers now believe that Irritable Bowel Syndrome (IBS) is caused by small intestinal bacterial overgrowth (SIBO). (10) A study performed at the GI Motility Center in Los Angeles in 2002 found that 71 percent of GERD patients tested positive for IBS—double the percentage seen in non-GERD patients being examined. (11) The high prevalence of IBS in GERD patients combined with the recognition that bacterial overgrowth causes IBS is yet another line of evidence suggesting that bacterial overgrowth is also a causative factor in GERD.
Final Comments
To summarize, low stomach acid contributes to bacterial overgrowth in the bowel which in turn can lead to carbohydrate malabsorption (due to decreased pancreatic enzyme secretion). Malabsorption of carbohydrates, as Dr. Robillard has pointed out, increases intra-abdominal pressure and causes GERD.
Where Dr. Robillard and I differ is that I believe low stomach acid is the primary problem with GERD, with carbohydrate malabsorption playing a secondary role. I do think that improper digestion of proteins can, in fact, lead to GERD, whereas Dr. Robillard states in his book that putrefaction of proteins is more likely to cause flatulence. This may be so in most cases, but I’ve seen several patients in my practice on very-low-carbohydrate diets who still experience heartburn, which improves upon restoring proper stomach acid secretion (which we covered in another article in this series). In the Part III of the series I discuss the connection between GERD and H. pylori, and further evidence supporting the theory that GERD is caused by bacterial overgrowth. Read on!
Better supplementation. Fewer supplements.
Close the nutrient gap to feel and perform your best.
A daily stack of supplements designed to meet your most critical needs.

I’m in a bit of a quandary. I have been suffering from reflux for years on and off. I’m not overweight but I do eat a fair amount of spicy food, which I’m reluctant to miss out on. I recently tried taking digestive enzymes with betaine hydrochloride, in line with the suggestions here. I have never experienced pain like it! I only took them twice and decided that it definitely wasn’t the answer for me. I’d rather suffer heartburn than that pain.
I suspect that I may have an ulcer. Would that cause reflux, though?
Giving erythromycin to people that already have stomach troubles? Sounds risky. Interesting read though.