

This is the second article in a series on heartburn and GERD. If you haven’t read the first one, I’d suggest doing that first.
The idea that heartburn is caused by too much stomach acid is still popular in the media and the public. But as Daniel pointed out in the comments section of the last post, anyone familiar with the scientific literature could tell you that heartburn and GERD are not considered to be diseases of excess stomach acid.
Instead, the prevailing scientific theory is that GERD is caused by a dysfunction of the muscular valve (sphincter) that separates the lower end of the esophagus and the stomach. This is known as the lower esophageal valve, or LES. The LES normally opens wide to permit swallowed food and liquids to pass easily into the stomach. Except for belching, this is the only time the LES should open.
Here’s the key point. It doesn’t matter how much acid there is in the stomach. Even a small amount can cause serious damage. Unlike the stomach, the lining of the esophagus has no protection against acid.
Free eBook
Learn More about Heartburn and GERD
Download this free eBook to discover the little-known causes of heartburn and GERD, and find out how to get rid of the problem forever.
"*" indicates required fields
I hate spam, too. Your email is safe with me. By signing up, you agree to our privacy policy.
We’ve Been Asking the Wrong Question
In an editorial published in the journal Gastroenterology, the author remarked: (1)
Treating gastroesophageal reflux disease with profound acid inhibition will never be ideal because acid secretion is not the primary underlying defect.
I couldn’t agree more. For decades the medical establishment has been directing its attention at how to reduce stomach acid secretion in people suffering from heartburn and GERD, even though it’s well-known that these conditions are not caused by excess stomach acid. Instead, the question researchers should have been asking is, “what is causing the LES to malfunction?” Since it is universally agreed upon that this is the underlying mechanism producing the symptoms of GERD, wouldn’t it make sense to focus our efforts here? That’s exactly what we’re going to do in this article.
GERD Is Caused by Increased Intra-Abdominal Pressure
It is well accepted in the literature that GERD is caused by an increase in intra-abdominal pressure (IAP).
For example, several studies have indicated an association between obesity and GERD, and one paper in Gastroenterology concluded that increased intra-abdominal pressure was the causative mechanism. (2, 3) But while I agree that all of the currently accepted factors play a role, I do not think they are the primary causes of the increased IAP seen in GERD.
The Two Primary Causes of Increased Intra-Abdominal Pressure
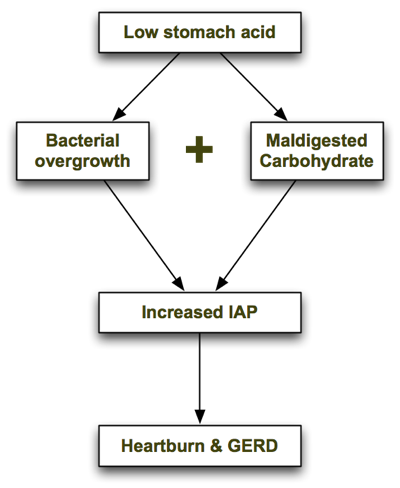
In his excellent book, Heartburn Cured, microbiologist Dr. Norm Robillard argues that carbohydrate malabsorption leads to bacterial overgrowth, resulting in IAP which drives reflux. Dr. Robillard makes a strong case that carbohydrate malabsorption plays a significant role in IAP, and I agree. But as I researched this issue I couldn’t help asking: what might be causing the carbohydrate malabsorption in the first place, and are there any other causes of bacterial overgrowth that may precede carbohydrate malabsorption? I believe the one answer to both of those questions is low stomach acid. Low stomach acid can contribute to both bacterial overgrowth (independently of carbohydrate intake) and carbohydrate malabsorption, as I describe below. In a nutshell, the process looks like this: Let’s look at each step in turn.
1. Low Stomach Acid Causes Bacterial Overgrowth
As I explain in the next article, one of the chief roles of stomach acid is to inhibit bacterial overgrowth. At a pH of 3 or less (the normal pH of the stomach), most bacteria can’t survive for more than 15 minutes. But when stomach acid is insufficient and the pH of the stomach rises above 5, bacteria begin to thrive. The gastrin knockout mouse, which is incapable of producing stomach acid, suffers from bacterial overgrowth—as well as inflammation, damage and precancerous polyps in its intestines. (4) It is also well documented that acid-suppressing drugs promote bacterial overgrowth. Long-term use of Prilosec, one of the most potent acid suppressing drugs, reduces the secretion of hydrochloric acid (HCL) in the stomach to near zero. In one trial, 30 people with GERD were treated with a high dose of Prilosec (40g/day) for at least 3 months. (5) Eleven of the 30 Prilosec-treated people had developed significant bacterial overgrowth, compared with only one of the 10 people in the control group.
2. Low Stomach Acid Causes Maldigestion of Carbohydrates
Stomach acid (HCL) supports the digestion and absorption of carbohydrates by stimulating the release of pancreatic enzymes into the small intestine. If the pH of the stomach is too high (due to insufficient stomach acid), the pancreatic enzymes will not be secreted and the carbohydrates will not be broken down properly.
Like what you’re reading? Get my free newsletter, recipes, eBooks, product recommendations, and more!
Bacterial Overgrowth + Maldigested Carbohydrates = GAS!
In Hearburn Cured, Dr. Robillard points out that though microbes are able to metabolize proteins and even fats, their preferred energy source is carbohydrate. The fermentation of carbohydrates that haven’t been digested properly produces gas. The resulting gas increases intra-abdominal pressure, which is the driving force behind acid reflux and GERD. From Dr. Robillard’s book:
According to Suarez and Levitt (17), 30 g of carbohydrate that escapes absorption in a day could produce more than 10,000 mL (ten liters) of hydrogen gas. That is a huge amount of gas!
When stomach acid is sufficient and carbohydrates are consumed in moderation, they are properly broken down into glucose and rapidly absorbed in the small intestine before they can be fermented by microbes. However, if stomach acid is insufficient and/or carbohydrates are consumed in excess, some of the carbs will escape absorption and become available for intestinal microbes to ferment.
Other Supporting Evidence
Dr. Robillard also argues that if gas produced by microbial fermentation of carbohydrates causes acid reflux, we might expect that reflux could be treated by either:
- Reducing bacterial overgrowth, or
- Reducing carbohydrate intake.
He points to two studies which demonstrate this. In a study by Pehl, administration of erythromycin (an antibiotic) significantly decreased esophageal reflux. (6)
In another study by Pennathur, erythromycin strengthened the defective lower esophageal sphincter in patients with acid reflux. (7) To my knowledge, there have only been two small trials performed to test the effects of carbohydrate restriction on GERD. Both had positive results. A small case series showed a significant, almost immediate resolution of GERD symptoms in obese individuals initiating a very-low-carb diet. (8) A more recent study found that a very low-carb diet decreased distal esophagus acid exposure and improved the symptoms of GERD. (9) Perhaps most importantly, the magnitude of the improvement was similar to what has been reported with treatment with proton-pump inhibitors (acid suppressing drugs).
Some researchers now believe that Irritable Bowel Syndrome (IBS) is caused by small intestinal bacterial overgrowth (SIBO). (10) A study performed at the GI Motility Center in Los Angeles in 2002 found that 71 percent of GERD patients tested positive for IBS—double the percentage seen in non-GERD patients being examined. (11) The high prevalence of IBS in GERD patients combined with the recognition that bacterial overgrowth causes IBS is yet another line of evidence suggesting that bacterial overgrowth is also a causative factor in GERD.
Final Comments
To summarize, low stomach acid contributes to bacterial overgrowth in the bowel which in turn can lead to carbohydrate malabsorption (due to decreased pancreatic enzyme secretion). Malabsorption of carbohydrates, as Dr. Robillard has pointed out, increases intra-abdominal pressure and causes GERD.
Where Dr. Robillard and I differ is that I believe low stomach acid is the primary problem with GERD, with carbohydrate malabsorption playing a secondary role. I do think that improper digestion of proteins can, in fact, lead to GERD, whereas Dr. Robillard states in his book that putrefaction of proteins is more likely to cause flatulence. This may be so in most cases, but I’ve seen several patients in my practice on very-low-carbohydrate diets who still experience heartburn, which improves upon restoring proper stomach acid secretion (which we covered in another article in this series). In the Part III of the series I discuss the connection between GERD and H. pylori, and further evidence supporting the theory that GERD is caused by bacterial overgrowth. Read on!
Better supplementation. Fewer supplements.
Close the nutrient gap to feel and perform your best.
A daily stack of supplements designed to meet your most critical needs.

Final article in the series is up.
Also, the entire series as well as recommendations for books and offsite articles can be found here.
Great series! After taking prilosec for over a year, my wife persuaded me that after having been on a low-carb diet for about the last 6 months of that time, my problem may well be gone. It was! Have had maybe a half dozen instances since (all due to overeating just prior to bed, and involved an abnormaly large carb intake). I used to have that many instances a week!
Smart wife! Aren’t you glad you listened to her? 🙂
Very nice article, Chris. That’s why drinking apple cider vinegar has been a popular home remedy for acid-reflux, for the reasons you explained. (2-3 teaspoon, with water if you feel it is too strong. It is good for blood stagnation type of chest pain too, even if it is not caused by heartburn)
Hi folks,
The next installment in the series is up: How your acid stopping drug is making you sick (Part A). Part B will be published on Monday or Tuesday.
Enjoy!
Oops, forgot to answer your question about FOS.
Yes, I think FOS will increase gas and heartburn in people with bacterial overgrowth. However, the question is whether this effect is temporary, as the bacterial flora in the gut rebalance, or ongoing. I don’t know the answer to that question.
Chris, I’m curious…
What does spicy food have to do with it? Do you know why it is that people experience more GERD symptoms when eating spicy foods?
Also curious about the FOS connection. Does that imply that FOS makes gas and heartburn worse?
Thanks for taking the time to put together all this info. 🙂
Sarah,
Spicy foods are often rated on surveys as among the worst culprits, but studies don’t actually support that notion. It’s difficult to isolate variables because nobody eats hot spices by themselves. They’re always eaten with food, and in many cases that food contains other ingredients like industrial vegetable oils and preservatives (i.e. kung pao chicken) that could irritate the stomach.
In some cases I suppose the spices alone could irritate the gastric lining, especially if someone has an ulcer or chronic stress has inhibited prostaglandin production and their mucosal barrier is compromised. But in that case it’s not the spicy food that is the problem – it just exacerbates the underlying condition.
what about salicylate intolerance? – spices are really high in sals
Hi everyone,
I’ve just published Part III of the series. This was an unplanned article based on a study I just came across yesterday that provides further evidence that GERD is caused by bacterial overgrowth, and examines the connection between GERD and H. pylori.
Enjoy!
We spent the last two years making dietary changes. The SCD seems to work great for us and now I’m looking into “fine tuning”. It’s funny/lucky, or however you want to put it, that your recent topics are covering things I have wanted to know more about, especially acupuncture and this. My son spent his first 8 mos of life on Zantec, so I have often wondered about this. I wonder if HCL could improve digestion. Is there a way to ask a doctor to check a small child for this?
I really enjoy the information and your writing style is great, easy to understand. I really appreciate all of this.
OK, if the burn returns I’ll pick up some 200mg HCL/pepsin thingies. So far, so good, but it’s only been 24hrs since I took the last Aciphex. I *hate* taking any sort of medication so getting off the PPIs would be a big win.
Admin: I drink kombucha daily and some days I eat full-fat “Fage” yogurt as I did this morning right out of the container. There’s a jar of Bubbe’s fermented raw pickles in the fridge I keep forgetting about.
Do PPIs have a permanent effect? I’m loathe to try HCL supplements at this point. Psychologically, I suppose, but I don’t ever want to revisit the searing pain of reflux ever again.
Forty2,
The effect is probably not permanent. However, there have been some reports that taking Prilosec can lead to achlorydia that can last more than two years after discontinuing the drugs. I completely understand your reluctance to try HCL. However, if it is low stomach acid that is causing your digestive problems, which seems likely, HCL could have a profound effect. Just make sure to take only 200 mg to start with, and do it before a meal. I’ve had several patients that have experienced remarkable results with HCL after years of heartburn and GERD.
Hi Chris, I have a question about these HCL supplements. I have been on omeprazole 40mg to 80 mg everyday for a few years because my endoscopy came back with gastritis, then shorty after I got esophagitis h. pylori and now I suffer from heartburn. I stopped the ppi for 2 days and the burning came back in my stomach and esophagus . I’ve been using an all natural remedy I found online called Siberian pine nut oil. how do these HCL work and how can I restore my stomach acid with the nutrients I’m loosing like (b12)? after stopping ppi’s for 2 days it came back strong. what do you suggest and what kind of diet would be ideal for me? Please get back to me the easiest way as I cannot find my way back to this site with a response. Thank you Amanda.
Amanda, tell me how are you doing, I have had the same simptoms as you.
Write to me at my email
DGL is amazing to help soothe. It’s a chewable so easy to take.
Other supplements that are very helpful:
– L-glutamine (find a quality brand like Pure)
– Aloe vera inner leaf (in small quantities- see label)
– Slippery Elm (make it into a ‘slurry’ as the powder forms a gel like substance when mixed with water. Leave sit for 10 or 20 mins until it becomes gel like and drink. It is soothing to the intestinal tract and stomach.
– Marshmallow tea (to a lesser degree but is also soothing for the gut)
*A brand called “Mucosaheal” is excellent too which combines many of these ingredients in a capsule.
Best of luck!
There’s a supplement in powder form called Glutagenics that contains l-glutamine, DGL and aloe all in one product.
One concern I have about DGL tablets is that the ones I have found all seem to contain sugar of some sort, or artificial sweeteners, or even both! Is dextrose something to be concerned about, that could sabotage a treatment plan, I wonder? Thanks.
Awesome article, Chris, and excellent explanations and references!
Thanks Mike!
Admin.
I am suffring from high acids.
I feel breathless.gas in stomach. Pain in abdomal.constpation.
Pain in chest.plz prescribe me some god way.
I have shown many doctors.they say its acid.
Prescribes me some medicine but nothing effects.
Also i feel very low .
Nd some time i feel weakness.my hands usualy sweats a lot.
Forty2,
My guess is your stomach acid is extremely low from the Aciphex. Try taking HCL w/pepsin capsules before meals. You might also try slowly increasing your intake of fermented foods (yogurt, kefir, raw sauerkraut, kombucha, etc.) to address the bacterial overgrowth. Constipation is almost always related to an insufficiency of healthy flora in the gut, which can also cause all of the other symptoms you describe.
admin: gas and pressure, eh? I went off Aciphex today. I’ve been on a very low-carb/hi-fat/hi-protein diet, and have felt tremendous pressure all along the lower rib cage (upper colon?) especially on my right side for the past week or so, have been farting like a tuba quartet and haven’t taken a crap in a week. Maybe going off Aciphex will hopefully knock something loose.
Tooearly,
When stomach acid is insufficient, putrefaction of protein can cause gas and increased intra-adbominal pressure. This could certainly affect your sleep. It’s possible your stomach acid is low or borderline low, and you’re not able to digest large amounts of protein.
Tim,
Bacterial overgrowth can cause hypochlorhydria, especially h. pylori. It’s estimated that more than 50% of people in the world are infected with h. pylori, so that’s probably the primary cause aside from PPI use. Studies indicate that h. pylori infection increases with age and is the cause of higher rates of hypochlorhydria in the elderly.
The medical test for low stomach acid is called the Heidelberg capsule test. It’s a small plastic capsule with measuring equipment that is swallowed and monitored via radio.
The “low-tech” way of testing stomach acid, which I’ll describe in the article on treatment, is to do an HCL challenge test. You take a 200 mg capsule of HCL w/pepsin before a meal. If you notice no burning, you increase to two capsules the next meal. Proceed until you notice a mild burning sensation, then immediately reduce your dose to the number of capsules that preceded the burning or heat sensation.
If one or two capsules causes burning, you either don’t have low stomach acid or your reflux is so severe that you won’t be able to take HCL until you get it under control. NOTE: do not perform this test if you have an active ulcer or a history of ulcer.
The bacteria don’t like coffee, but if she has milk and sugar in it they love that. Coffee is high in tannins, which can cause indigestion.
Chris,.
I read that you mentioned not to perform the “low-tech” test if someone had a history of Ulcer . I had duodenal ulcer in 2012 caused by H Pylori. So I just recovered from it recently but what remains is the constant gnawing pain, bloating, pressure, and sometimes even shortness of breath. My doctor prescribed PPI which is giving me temporary marginal relief. Since i am one of those excluded to take HCL due to history of ulcer, what are my remedies?
My son suffered from GERD and took prilosec and tums like they were candy. He also smoked Vapor cigarettes that had PG and VG and nicotine in them. Could this cause a problem for someone with GERD?
Thanks for your response.
well written. I imagine that there is incredible variability in how each of our guts responds to different diets. Big protein meals for supper have always made me sleep poorly.
Great article. I have a lot of questions 🙂
Except medicine, what can cause low stomach acid? I know there are people who had GERD but hadn’t taken any meds. Could it be low levels of minerals, proteins, fats? Or is it perhaps the bacterial overgrowth itself?
How do one test for low stomach acid?
I have a relative with GERD. The reflux happens when she drinks coffee. Do the bacteria like coffee? What other non-carb intense foods can cause reflux and why does this happen?
Very good article.
My acid reflux (very bad even at a young age) seemed to get worse during times in my life when (i) I weight lifted and (ii) drank a lot of beer. Weight lifting can cause IAP as does the bloating from beer (and maybe some carb malabsorption too).
I’ve considered going very low carb to avoid reflux but I think the other health costs weigh against it (but that’s another whole conversation).
Thanks for your very thoughtful essay.
Good catch there, Daniel.
I think that studies will make a correlation between weight lifting (or personal caregivers deadlifting their charges) and hiatal hernias. Further that there is comorbidity for hiatal hernias and GERD. It is more likely that a person with a hiatal hernia has GERD than a person without the ailment.
While I was quite prepared to be “underwhelmed” with Mr. Kresser’s article, I’m quite impressed. Most of the article has solid scientific underpinnings if not rational assumptions and correlations. I think it’s important to bear in mind the comparative methodologies of differential diagnosis and causation assessment; but in this case I think Occam’s razor cuts to the heart of it. The underlying problem is always the LES, yet that is not what doctors will diagnose, nor what insurance companies will pay to treat.
While I’m unaware of a “test” that confirms IBS, as Chris alluded to here, I do know that there is growing acceptance of the hydrogen breath test (HBT) as an indicator of SIBO. I suspect that SIBO, IBS, and GERD can all work independently, in concert or synergistically and that hiatal hernias may help reinforce a diagnosis. While I’ve not read anything that suggests that antibiotics help repair or strengthen the LES, antibiotics have proven to reduce or eliminate the symptoms of GERD. I agree with the conclusion that one would better approach these problems by reducing carbohydrates while tapering off of proton pump inhibitors. To prove a diagnosis of SIBO by undergoing prolonged treatment with antibiotics may not be the best first step. If undergoing treatments of broad spectrum antibiotics, one must be prepared to immediately reintroduce mega-doses of pro-biotics, lest an antibiotic resistant strain of bacteria overgrows.
Thanks for the good information and sources! I look forward to the next article.
I never had acid reflux until I started drinking Lifeway Kefir liquid yogurt. I started drinking 4ozs every morning since Nov. 2013 for two weeks. I suddenly got acid reflux so bad it was incredible. I stopped the kefir, but continued the severe reflux for four months. Finally I got a little relief then one day a bought a single yogurt and this problem started all over again, Now I can’t have any yogurt at all. I am positive the kefir ruined my digestive system . So much for a good thing.
Me too! I’m convinced kefir set me off with all kinds of digestive problems! It really didn’t do me any favours, and I’m now taking a trade off antibiotics to try to stop the well long diahrrea I’ve had!
Please address kefir Chris, so many of us try it thinking were doing something good and end up worse off! Why does kefir do this?
I too believe Kefir started my reflux and digestion issues. I was making my own and was taking it for a couple of months, I think it may have caused an overgrowth of bacteria
Well Chris, more interesting info. Some of this I was familiar with, but found the studies involving the use of antibiotics to treat the bacteria and resulting GERD symptoms especially strengthening the LES intrigues me.
Since I’m still in the early stages of overcoming this condition, could I possibly benefit from a course of antibiotics? And if so, is there an alterntive to erythromycin? It’s been years since I’ve taken any, but got horrible stomach pain when I did. I think it’s just a basic broad spectrum antibiotic, isn’t it?
Secondly, I sensed that dairy was a problem for me due to the milk protein. In particular, it aggravated my asthma because it does cause production of mucous. However, I have recently discovered raw milk and seem to not experience problems with it; either mucus production or reflux. I’m wondering as in the case of yogurt, if the naturally ocurring friendly bacteria in raw milk pre-digests most of the lactose that feeds the bad bacteria in the gut. In addition, perhaps those friendly bugs help keep some of the bad bugs in check that would produce the gas. Your thoughts?
Hi Kim,
I’m not sure if I mentioned this, but I am planning a follow-up to this series on the connection between asthma and GERD.
To answer your question, one of the reasons raw milk is superior to pasteurized milk is that it has lactase in it. Lactase is the enzyme we need to digest lactose, the sugar in milk. In non-dairy consuming societies, lactase production usually drops about 90% during the first four years of life (after weaning), although the exact drop over time varies widely.
Pasteurization kills lactase. This is why so many people have trouble digesting pasteurized milk. But those same people can often digest raw milk without a problem, because it has lactase in it.
The probiotics in yogurt (as well as kefir, sauerkraut, kombucha, kim chi and other fermented foods) can be helpful in re-establishing healthy gut flora.
Before resorting to antibiotics, I would try a period of time with a grain-free, very low-carb diet (< 30g/day) combined with an increase in probiotic intake and HCL w/pepsin supplements. It's important to proceed slowly as you increase the probiotics, because moving too fast can cause gas, bloating and intestinal discomfort.
What’s your take on digestive enzymes supplements?
They can be helpful for short-term use, but ultimately acidifying the chyme in the stomach (via HCL supplementation) should produce the same effects and save you $$.
I have found Aloe Vera Juice to be extremely effective with treating GERD.
i used to drink lemon with cucumber, celery and kale every morning and how come i have LPR? is it better to take 1 tsp of apple cider vinegar in the morning to increase stomach acid? i stop taking prilosec today and i hope it’s better without it. you mentioned something about yogurt, can i have the non flavored yogurt instead? in this way it’s not loaded with sugar.
One more thing: there is evidence that raw milk can prevent asthma from developing in children. I haven’t seen any studies on whether it can actually treat or cure asthma, but it’s certainly possible.
When my oldest son was transitioning to whole milk at 1 year old, he had problems digesting it. He experienced diarrhea and acid reflux. I switched him to soy which he had no problem with. After a few months I tried milk again, this time organic. He was able to digest organic milk, but not regular whole milk. I have often wondered why this was.
I too can digest organic milk but not ‘normal’. It all comes down to synthetic chemicals, from the sprays used on their food, injections for medicine etc and any other additives put into the milk along the way. Even any highly processed milk will come in to more – the more machines they have to go through the more ‘cleaning’ chemicals etc they will pick up. When I went organic in my whole diet my 20 years of asthma, allergies, arthritic pain, anxiety, depression, bad skin, fatness, PCOS and more all disappeared. Synthetic chemicals are ruining our health (especially endocrine disruptors) and our beautiful world 🙁 I get the most horrible reflux whenever I add them back to my diet and my asthma returns immediately. Especially with food additives like MSG.
Great article. I will wait for the followup.
Read Dr Hiromi Shinya and get your stomach and intestines healthy
The Enzyme Factor
i have low stomach acid and anti body antiparietall cells they had to give me b 12 shots now i take sublingual i find that my body absorbs Methylcobalamin better which i found i still had low iron anemia which i was blaming the whole time on aunt flow but i had n heavy bleeding to have a low iron that was going up and down in numbers all the time.I did my own surfing internet and began supplementing also i felt a difference with digestive enzymes that break down protein milk carbs.Now im trying to recover no carb intake.Im trying to find a good probiotic that would work for me.Keep in mind i did have test done that show i had low stomach acid. Remember if a test show negative for gluten or Celiac you can still be sensitive to gluten.I had t go t s man doctors until i got tested for low stomach acid. wish you all health i know how you all feel.
I found your article by doing a search to see the antibiotic im taking for a dental reason stopped the last of my GERD and heartburn! I had been taking 20mg of Omeprazole daily for 13 years. I wanted off but its really hard to get off. I managed to get down to 5 mg a day, but no further. Then I get zithromyacin from my dentist, and noticed I wasnt feeling the burn. At 5 mg omeprazole I was still having to take a 75mg Ranitadine and several OTC chewables daily. Now , while on antibiotic, Im feeling different! Today will be 2nd day of just Ranitidine. Im hopeful that I wont have to go back to the Omeprazole after the course of antibiotics! Thanks for this article!
The ongoing saga of heartburn… I found that my heartburn improved after taking an antibiotic prescribed for another ailment. It led me to this website and gave me some hope that I could get better. Although progress is slow, it is consistent and positive. One thing that I did do lately was a parasite cleanse. I did the cleanse twice for 15 days with a 5 day break in-between the two courses of the cleanse. I ate normally and even drank alcohol. I would suggest to anyone who has heartburn to at least try a parasite cleanse. A holistic practitioner friend recommended that I do it with a homeopathic kit, which I will do next. However, it cost twice as much as the herbal cleanse, so I thought I’d try that first. I’m finding that I am much improved. Now I will start upping my probiotic.
One other clue I had that I might have parasites is that this summer I had a gin & tonic. Tonic has quinine which is used to fend off malaria. I actually felt better after drinking a gin and tonic — and I don’t think it was the gin 🙂 — although that could be good, too 🙂
Hi All,
I was forwarded this site after recent discussion with a friend having acid reflux issues. She has now followed my suspicions and after two days is feeling better.
12 months ago I decided to make a life change and undertake ” The Fast Diet” by Dr Michael Mosley in the UK. My wife and I both started the process of reduced calorie intake two days a week. Due to the calorie count of a few slices of bread, I went cold turkey and cut out all grain products to see how I felt. Within 1 month I was able to come off 40mg Somac ( over 15 years daily use). Suddenly all my reflux problems disappeared, irritable bowell syndrome gone, permanent bloating and lethargy gone, constant thrush gone. I am convinced my long standing medical issues have been grain related and I have stumbled onto this life changing process purely by accident. I am absolutely convinced the medical profession prefer to treat symptoms instead of the underlying issues. I recently had a coeliac test which proved negative but after removing bread / cereals from my diet, I feel 30 years younger and 14kg lighter. After reading the information related to this site my suspicions and now beliefs are proven medically.
Good luck to all reading this – quit bread and throw the pantaprazole in the bin. You will feel better for it. Don Barker
Whangarei New Zealand