

This is the second article in a series on heartburn and GERD. If you haven’t read the first one, I’d suggest doing that first.
The idea that heartburn is caused by too much stomach acid is still popular in the media and the public. But as Daniel pointed out in the comments section of the last post, anyone familiar with the scientific literature could tell you that heartburn and GERD are not considered to be diseases of excess stomach acid.
Instead, the prevailing scientific theory is that GERD is caused by a dysfunction of the muscular valve (sphincter) that separates the lower end of the esophagus and the stomach. This is known as the lower esophageal valve, or LES. The LES normally opens wide to permit swallowed food and liquids to pass easily into the stomach. Except for belching, this is the only time the LES should open.
Here’s the key point. It doesn’t matter how much acid there is in the stomach. Even a small amount can cause serious damage. Unlike the stomach, the lining of the esophagus has no protection against acid.
Free eBook
Learn More about Heartburn and GERD
Download this free eBook to discover the little-known causes of heartburn and GERD, and find out how to get rid of the problem forever.
"*" indicates required fields
I hate spam, too. Your email is safe with me. By signing up, you agree to our privacy policy.
We’ve Been Asking the Wrong Question
In an editorial published in the journal Gastroenterology, the author remarked: (1)
Treating gastroesophageal reflux disease with profound acid inhibition will never be ideal because acid secretion is not the primary underlying defect.
I couldn’t agree more. For decades the medical establishment has been directing its attention at how to reduce stomach acid secretion in people suffering from heartburn and GERD, even though it’s well-known that these conditions are not caused by excess stomach acid. Instead, the question researchers should have been asking is, “what is causing the LES to malfunction?” Since it is universally agreed upon that this is the underlying mechanism producing the symptoms of GERD, wouldn’t it make sense to focus our efforts here? That’s exactly what we’re going to do in this article.
GERD Is Caused by Increased Intra-Abdominal Pressure
It is well accepted in the literature that GERD is caused by an increase in intra-abdominal pressure (IAP).
For example, several studies have indicated an association between obesity and GERD, and one paper in Gastroenterology concluded that increased intra-abdominal pressure was the causative mechanism. (2, 3) But while I agree that all of the currently accepted factors play a role, I do not think they are the primary causes of the increased IAP seen in GERD.
The Two Primary Causes of Increased Intra-Abdominal Pressure
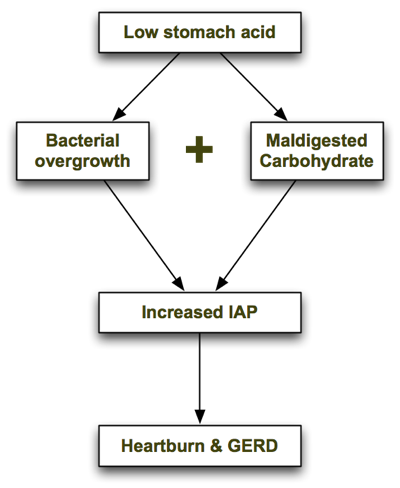
In his excellent book, Heartburn Cured, microbiologist Dr. Norm Robillard argues that carbohydrate malabsorption leads to bacterial overgrowth, resulting in IAP which drives reflux. Dr. Robillard makes a strong case that carbohydrate malabsorption plays a significant role in IAP, and I agree. But as I researched this issue I couldn’t help asking: what might be causing the carbohydrate malabsorption in the first place, and are there any other causes of bacterial overgrowth that may precede carbohydrate malabsorption? I believe the one answer to both of those questions is low stomach acid. Low stomach acid can contribute to both bacterial overgrowth (independently of carbohydrate intake) and carbohydrate malabsorption, as I describe below. In a nutshell, the process looks like this: Let’s look at each step in turn.
1. Low Stomach Acid Causes Bacterial Overgrowth
As I explain in the next article, one of the chief roles of stomach acid is to inhibit bacterial overgrowth. At a pH of 3 or less (the normal pH of the stomach), most bacteria can’t survive for more than 15 minutes. But when stomach acid is insufficient and the pH of the stomach rises above 5, bacteria begin to thrive. The gastrin knockout mouse, which is incapable of producing stomach acid, suffers from bacterial overgrowth—as well as inflammation, damage and precancerous polyps in its intestines. (4) It is also well documented that acid-suppressing drugs promote bacterial overgrowth. Long-term use of Prilosec, one of the most potent acid suppressing drugs, reduces the secretion of hydrochloric acid (HCL) in the stomach to near zero. In one trial, 30 people with GERD were treated with a high dose of Prilosec (40g/day) for at least 3 months. (5) Eleven of the 30 Prilosec-treated people had developed significant bacterial overgrowth, compared with only one of the 10 people in the control group.
2. Low Stomach Acid Causes Maldigestion of Carbohydrates
Stomach acid (HCL) supports the digestion and absorption of carbohydrates by stimulating the release of pancreatic enzymes into the small intestine. If the pH of the stomach is too high (due to insufficient stomach acid), the pancreatic enzymes will not be secreted and the carbohydrates will not be broken down properly.
Like what you’re reading? Get my free newsletter, recipes, eBooks, product recommendations, and more!
Bacterial Overgrowth + Maldigested Carbohydrates = GAS!
In Hearburn Cured, Dr. Robillard points out that though microbes are able to metabolize proteins and even fats, their preferred energy source is carbohydrate. The fermentation of carbohydrates that haven’t been digested properly produces gas. The resulting gas increases intra-abdominal pressure, which is the driving force behind acid reflux and GERD. From Dr. Robillard’s book:
According to Suarez and Levitt (17), 30 g of carbohydrate that escapes absorption in a day could produce more than 10,000 mL (ten liters) of hydrogen gas. That is a huge amount of gas!
When stomach acid is sufficient and carbohydrates are consumed in moderation, they are properly broken down into glucose and rapidly absorbed in the small intestine before they can be fermented by microbes. However, if stomach acid is insufficient and/or carbohydrates are consumed in excess, some of the carbs will escape absorption and become available for intestinal microbes to ferment.
Other Supporting Evidence
Dr. Robillard also argues that if gas produced by microbial fermentation of carbohydrates causes acid reflux, we might expect that reflux could be treated by either:
- Reducing bacterial overgrowth, or
- Reducing carbohydrate intake.
He points to two studies which demonstrate this. In a study by Pehl, administration of erythromycin (an antibiotic) significantly decreased esophageal reflux. (6)
In another study by Pennathur, erythromycin strengthened the defective lower esophageal sphincter in patients with acid reflux. (7) To my knowledge, there have only been two small trials performed to test the effects of carbohydrate restriction on GERD. Both had positive results. A small case series showed a significant, almost immediate resolution of GERD symptoms in obese individuals initiating a very-low-carb diet. (8) A more recent study found that a very low-carb diet decreased distal esophagus acid exposure and improved the symptoms of GERD. (9) Perhaps most importantly, the magnitude of the improvement was similar to what has been reported with treatment with proton-pump inhibitors (acid suppressing drugs).
Some researchers now believe that Irritable Bowel Syndrome (IBS) is caused by small intestinal bacterial overgrowth (SIBO). (10) A study performed at the GI Motility Center in Los Angeles in 2002 found that 71 percent of GERD patients tested positive for IBS—double the percentage seen in non-GERD patients being examined. (11) The high prevalence of IBS in GERD patients combined with the recognition that bacterial overgrowth causes IBS is yet another line of evidence suggesting that bacterial overgrowth is also a causative factor in GERD.
Final Comments
To summarize, low stomach acid contributes to bacterial overgrowth in the bowel which in turn can lead to carbohydrate malabsorption (due to decreased pancreatic enzyme secretion). Malabsorption of carbohydrates, as Dr. Robillard has pointed out, increases intra-abdominal pressure and causes GERD.
Where Dr. Robillard and I differ is that I believe low stomach acid is the primary problem with GERD, with carbohydrate malabsorption playing a secondary role. I do think that improper digestion of proteins can, in fact, lead to GERD, whereas Dr. Robillard states in his book that putrefaction of proteins is more likely to cause flatulence. This may be so in most cases, but I’ve seen several patients in my practice on very-low-carbohydrate diets who still experience heartburn, which improves upon restoring proper stomach acid secretion (which we covered in another article in this series). In the Part III of the series I discuss the connection between GERD and H. pylori, and further evidence supporting the theory that GERD is caused by bacterial overgrowth. Read on!
Better supplementation. Fewer supplements.
Close the nutrient gap to feel and perform your best.
A daily stack of supplements designed to meet your most critical needs.

Hi Chris,
I have been suffering with Acid Reflux very badly since the summer, but last year had to take Ferrous iron as I was anaemic. Do you think that low stomach acid might have been the cause of the anaemia? I had a colonoscopy and all was fine there and was tested for Coeliac disease and that was fine, so they decided that my periods must be heavy. I think that they were wrong!
I am quite worried about it now, as I wonder what other nutrients I have not been absorbing. I have read Dr.Wrights book with great interest, and as I live in England (where H2, PPI’s are also given out like sweeties) there is no way to have your stomach acid levels assessed, the Heidelberg capsule is not used by UK doctors. (I emailed Heidelberg to find out!). So I decided to take the plunge and start taking Betaine HCL with Pepsin – after being prescribed by the doctors one lot of omeprazole for 2 weeks and one lot of Zantac (about a month later), both of which made me feel worse. Also I am following Dr.Wrights ideas by supplementing with vitamins, DGL before eating and am about to start taking digestive enzymes too. I have ordered an organic kefir starter kit to start to encourage the good bacteria. However, I am definitely feeling quite unwell (was before the HCL) and am still having some reflux and heartburn. I am very thin already and am worried about reducing carboydrates as I am worried that I will lose more weight. I am taking on average 5-6 HCL capsules (648mg) with every meal. If I take them towards the start of the meal I have no burning or warming sensation at all. My tongue is coated with white and I am generally feeling very exhausted, with huge bags under my eyes! I am nearly 47 years old and feel about 80. Last year I was very fit, a ten mile a week runner who only realised my iron levels were low when I lost all stamina. On the 16th December I am having an endoscopy to look at the esophagus but feel that this will only make my doctors say “You need acid blocking drugs” when I am sure the reason is otherwise. I have been on 5/6 capsules for a week, and the previous week worked up from one to two to three etc over the period of that week. I have stopped at 5/6 as Dr. Wright recommends that 5-7 seems to be the optimum number. I know that I am only 2 weeks in, but is there any idea how long it will take to kick in? I think my reflux is slightly lessened which is good, and the belching is lessened but still not gone. My lower guts seem to have given up and I am very constipated which is a nightmare. I would be very grateful if you could give me an idea of which carbohydrates to avoid..are all veg and fruit alright to eat? I’m a little muddled and more than a little sorry for myself! Thank you.
Yes, HCL (stomach acid) is required for iron absorption, so low stomach acid can certainly cause anemia. Restricting carbohydrates (of all types) to less than 50g for a period of time can be helpful.
Thank you, I will continue with the HCL Pepsin and cut down the carbohydrate..and stop with any grains, try and introduce good bacteria. I notice that you advocate a Paleo approach to diet, funnily enough I had started to embark on this when the reflux started – maybe a sign that the low acid in my stomach just was not able to cope with the higher levels of protein were introduced? Thank you for all your invaluable advice, it is great to hear a voice that is looking at ALL the evidence to provide answers, rather than following the conventional medicines route of PPI’s and acid blockers.
Hi, I have absolutely been put through the ringer. I was having throat pain almost 6 months ago. To make a short story of the affair I went through a normal doctor, an ENT, and finally a GI. I have been given a z-pac, antihistamines, prilosec, prevacid, carafate, gaviscon, In that order. I had burped a few times before this ordeal and food would come up. I never really thought about it till the throat problems.I had loose stools from time to time (ate lots of cereal, fats (cheese), carbs (bread), and popcorn) also I always get sick from eating really greasy or sugary food (runs in the family) but otherwise no pain or bloating etc. After being put on these meds I can’t eat more than a bite without feeling nauseous, bloated, etc. I had been having gas for a few days that smelled absolutely rotten from both ends (It is embarrassing however I have never produced anything that rancid before). I felt mildly normal while on the last set of meds (gaviscon and carafate) until I stopped taking them to gauge the rebound effect and it is excruciating. One of these two meds is what has caused the smelly death farts and what I assume is gas pain and/or acid burning from the food in my stomach putrefying. The gas and continued stomach upset are what finally prompted me to disregard my doctors advice. So now I am taking something called ‘probiotic multi-enzyme by nature valley’ and it is chocked full of enzymes: Calcium 144mg, Phosphorus 110mg, Betaine Hydrochloride 100mg, Pancreatin 100mg, Amalase 50 mg, Protease (papaya extract)50mg, Bromelain (600GDU per gram) 25mg, Papain (papaya extract) 25mg, Pepsin 25mg, Ox Bile25mg, Lipase 25mg, Cellulase25mg, Lactobacillus Acidophilus 1 billion. The death gas is gone but otherwise I am not noticing any immediate relief upon taking these enzymes. I have been on them for a little over three days. I want to take more HCL on its own but my stomach constantly HAS a burning sensation, I don’t want to take more than I should (if I even need it) but I am having trouble coming up with a way to gauge the burn. Endoscopy no ulcers, negative for H. Pylori. I am also leaning toward a possibility of food intolerance.
Hi Samantha, I’m also in the uk and had a similar experience to you – I wondered how you had got on in the intervening 18 months?
I was plagued by indigestion and gas for a number of years before the serious reflux symptoms started. I’ll never forget the first time I felt that violent, stabbing pain. For a couple weeks I was afraid to eat – especially in public for fear the pain would strike and I’d be buckled over, unable to control myself.
My doctor prescribed Tagamet, which I took before every meal for months.
In 2003 I went on a low carb diet for weight loss (I was about 50 lbs overweight), and at some point along the way I ran out of Tagamet. I ate rather cautiously for a few days but felt pretty good. Intrigued, I bought more Tagamet but decided I’d wait to take it until I experienced symptoms. I never opened the box of Tagamet, and threw it away a couple years later.
It’s been 8 years now and my GERD has never come back. I still eat moderately low carb most of he time. I always attributed the disappearance of my GERD to low carb but never knew for sure. It all makes perfect sense now!
THEY HAVE SAID THAT WITH A SCOPE THAT MY VOCAL CORDS ARE SWALLEN AND MY TONSILETS –I HAVE HAD MY TONSILS OUT WHEN I WAS 12 – NOT SURE WHAT TONSILETS ARE. I AM A SINGER AND HAVE NOT BEEN ABLE TO SING FOR MANY YEARS DUE TO CLEARING OF THE THROAT, AND SWELLING LIKE IN THE THROAT WHEN DOING SO. I USUALLY DON’T HAVE HEART BURN WHERE YOU CAN FEEL IT, BUT ONCE IN A WHILE DO HAVE THE REFLUX THAT LETS FLUID COME UP INTO THROAT AND MOUTH. sO DOES THIS SOUND LIKE (GERD) AND WHAT MIGHT I HAVE TO DO TO STOP THIS.
JUDY L.
Hi Chris
I just wanted to let you know I am doing much better on the Acid Reflux, and Haven’t taken any of the Meds since I started taking the Vinegar in the a,m and the DGL and spices that you recomended to me.
I am soooo thankfull for your Great Advice.
Waiting to read #3 in this subject. Keep them coming.
Many Many Thanks Rosalyn
Hi Chris
I loved your article. It is simply great. I want to learn more about alternatives medicine now.
I have acid reflux. I want to learn more about I started having it when I was about 30 years old and had frequent heartburn. I did few treatments with drugs that doctors prescribed me but it never worked so I started taking omeprazol on my own. It has kept my heartburn away but I am having too much bloating and my bowel movement is not good. I have taken it for about 2 years. I did an endoscopy last month and my doctor said my esophagus lining was fine and he recommended me to continue with omeprazol. I try to eat healthy as possible but before I started taking the anti acid it made very hard for me to eat. If I had garlic, for example it made sick. I was afraid to eat. I did not know that carbohydrates were the food to avoid until now. In the brochure that my doctor gave me it says that I should avoid acidic foods, fattening foods, and caffeine and dairy. I tested for the H. Pylori a year ago and came negative. So I am going to stop the anti acid now because I know I damaging myself with it. Do you have any suggestions besides decreasing my carbohydrates intake. I eat my carbohydrates more from fruits, legumes, leafy vegetables and whole wheat products.
Hello Chris,
Thank you very much for the very informative article!
It would be great to get your suggestions on how to increase stomach acidity (besides following the low carb diet).
I find that raw milk, vitamin C and ground mustard seeds work really well for me, but I can’t really take them with each meal. I’d like to stay away from the HCI supplements if possible.
Any thoughts?
Thanks,
Beth
Hi Kris!
I First want to say, I enjoyed reading your articles and hope to try some of your changes soon. My case seems to be a little different and thought you may be able to provide some insight. Had an upper endoscopy three years ago which resulted in diagnosis of Gerd and Hitias Hernia. Tried a variety of medications. Was still having other symptoms to include chest discomfort, belching, gas etc. Recently had a 24 hour PH Probe test done as well as motility on esophogus. I was taking Prevacid twice a day prior to test. Test revealed that despite me taking medication I still had higher than normal acid as well as bile reflux? I was told to up my dose of Prevacid. I haven’t noticed any changes since the increase in dosage. Additionally I recently had bloodwork done to show enemia and low vit D. My gastro now wants to do another endoscopy to biobsy for allergies or celiac? My questions are, since I seem to have higher acid and not lower, is it still possible to have the bacteria that is causing the preasure or maybe the bile? Secondly is there any correlation between celiac and acid reflux or esophogeal issues that you are aware of?
I have hit a Road Block.
I have High Blood Presure and was told by Karen that is in charge of the Suppliment Isle at the store where I work, that I shouldn’t really take the DGLs as it may put up the BP.
Is that right??? Nd if so what sould I do go back to doing the Vinegar befor eating.????
Thanks Rosalyn
Rosalyn, I hope it’s not too late to reply to your question about DGL. It is SAFE to take. It does NOT raise blood pressure. The reason it is safe is because the natural licorice has been “denatured” to remove the substance that causes the kidneys to retain water and thereby raise blood pressure. (Notice that DGL stands for DE-Glycyrrhizinated Licorice.) If you’re still not convinced, do a Google search on DGL.
I always keep a bottle on hand.
All the best,
Pat
Thank you I am in the middle of trying to read this stuff.
It is a lot to read. But I have learnt a couple of things already.
Always eat Bubbies–Kombucha we sell and tried it, Yuk, but I will try to drink it again–We sell DGL.
I will get some of the Herbs, and try 5 drops in water. How often should that be a day.
Thank you so very much Rosayn
Hi I just joined your email list.
A friend told me about taking vinegar before a meal, I started out doing it before every meal, for a few days.
Now I am doing it before Breakfast and Dinner.
Which is the right way or am I completely wrong in both ways.
I work at a Health food store as Cashier. And a friend told me to take Papaya Tabs when I get the heart burn in between, and it has also helped me.
I was taking the Meds for about 7 to 10 years, and I am determined to not take any more, altho they did work for me and after finding out what they do to your body, I really want to quit them.
Any Help you can give me will sure be appreciated. Thank you so much, Rosalyn
Make sure to check out all of the articles in this series: https://chriskresser.com/heartburn
Great article, Chris. As a Nutritional Therapist, I’ve found starting people on jsut a low carb diet (or in some cases just removing gluten) often reduces symtpoms of heartburn and GERD. If things don’t improve or improve only mildly, I’ll then bring in the HCl. No need to supplement if diet alone can take care of the problem!
Chris,
What about hiatal hernias as a cause for GERD? What is the current information you have about this?
I came across several studies which show that there exists an unbuffered layer of “acid pocket” post meals which could be responsible for reflux symptoms. Here are the links:
https://www.ncbi.nlm.nih.gov/pubmed/11606490
https://gut.bmj.com/content/57/3/285.extract
Here is a latest one done last year:
https://www.ncbi.nlm.nih.gov/pubmed/19651625
If these findings are true then, woudnt increasing stomach acid be a bad idea? since the problem may not be related to low stomach?
Shyam
I bet people note spicy food on surveys because the reflux is that much more painful. The one time I saw a digestive disease doctor (who was useless) I completely gave him the bitchface when he suggested not eating spicy foods. I make very spicy foods at home and I already knew that raw jalapeno and crushed red hot peppers, etc, did not exacerbate my symptoms. I’m glad the science has borne that out.
The one exception is when I had an active ulcer. OW!!
Btw, Doc, since I had a prior H. pylori infection (which the doctors I went to would not give me antibiotics for–I thought antibiotics were standard of care?–though they did waste my money on a “magic 8 ball says ‘results murky'” gall bladder ultrasound), should I undergo a course of antibiotics? My digestion has been slowly deteriorating and I finally cut out wheat/barley/rye and all but small amounts of un-nixtamalized maize (i.e. corn meal) from my diet. (To clarify, I am eating nixtamalized maize, aka masa, products, such as tortillas. They go down like butter!) This did 86 the GERD symptoms (less than a week–much faster than Prilosec), but you have me worried about my acid production.
I have been diagnosed with GERD, and, through an endoscopy, was told that I have a small hiatal hernia. Isn’t that a structural issue that prevents the LES from functioning properly? Is there anyway, other than medication, that I can manage my reflux?
In your summary – reduce bacteria AND limit carbs. Yes I live on fiber carbs for IBS/constipation prone and dairy for osteoporosis and recently have really started bloating and having gas. I’m a senior citizen who now has time to eat and I enjoy it and hate taking pills. I’ve always been convinced that what we eat makes us sick and what we eat will make us well. If it’s not carbs does that just leave meat?? And how do we reduce the bacteria? I take a lot of GAS X and every morning I take a Jarrodophilus with FOS capsule. I also test “allergic” to brewer’s yeast and baker’s yeast which none of the Dr.s I go to recognize. I need a Holistic, Geriatric Physican that specializes in diet. Thanks for your help.
The natural human diet is high in saturated fats (65%), relatively low in carbs (20%) and moderate in protein (15%). So, yes, meat and traditional fats make up the bulk of calories, but by weight ends up being 60% plants (starchy tubers, fruits, berries & veggies) and 40% animal foods (fatty meats, seafood, eggs, healthy fats). You reduce the bacteria by reducing the carbohydrate content, and by consuming fermented foods.
Im ready to give up. I’ve been having really bad stomach issues I dont get the typical burn associated with heartburn I just tast acid then I get bloated and then I feel like I can breathe. I was diagnosed with h.pylori and mild acid reflux about a year ago and its much worse now. Nothing helps and im scared to eat. For about 2 weeks I’ve been on a very low carb diet and today I had half of a bagel and then it happened I got bloated tasted the acid and couldn’t breathe. I cant live like this and I need help. I hope you can help me. Thank you
Do you know much about gastroparesis? I saw that it could also present with my same symptoms, but I don’t know how common it is. I sometimes get heartburn, nausea(less frequently and not necessarily after eating),bloating and belching after a meal, and sometimes it comes or continues up until a few hours after I’ve ate! Are those symptoms still a normal case of indigestion/ low stomach acid? Everything started after I had a course of antibiotics with prednisone. First was the gastritis, which started out as major belching, then ended up burning badly, which I went on Prilosec for. I also have bowel troubles sometimes. I’m worried of rushing into something and somehow making myself worse. In your opinion, should I be worried about another cause?
Brittany,
Your symptoms are what they call “non-specific”, which means they could be caused by any number of things. Based on your history (i.e. they started after antibiotics & steroids), my guess is they’re due to intestinal dysbiosis. Both antiobiotics and steroids have a profound impact on the gut flora. Dysregulated gut flora can cause IBS, IBD, GERD and several other digestive conditions. The “three R” therapy I described in my GERD articles would still apply as a general strategy, but you may want to seek out help from someone familiar with treating GI problems with natural approaches. I use a stool or breath test for H. pylori. I’m not certain of the accuracy of the blood tests.
I have the same exact problem i had a severe sinus infection and was treated with prednisone and antibiotics in the 6th grade and have had severe acid reflux/indigestion/bowelproblems/ and swallowing eversince. I can’t lay down at night or play sports anymore im in 10th grade now and im getting really to wonder what i can do, my symptoms got worse after working out but its really stressing me out and taking a toll on my life. Any suggestions? my only tests i havent done is barium swallow/gi series .
thank you! will order some HCL for the heartburn and keep reading for the other stuff
Hi Chris,
I have been reading your very informative blog for a while, first found it through the podcast about fish oils. I see you are yet another advocate of a low carb diet. From everything i read here and everywhere it seems like all my problems (hypoglycemia, heartburn weight gain etc) should be cured by a low carb diet but in reality I didn’t experience any of these problems until after the first time I tried a low carb diet. Every time I lower my carbs (am trying to lose 10lbs right now) I have gas, heartburn, hypoglycemia, mood swings, weight gain etc. I think it is from the healthy fats in the fish and olive oil on the veggies so the obvious answer would be to switch back to higher carbs but I am fearful because of everything i read suggests the opposite. I did go to the dr but they really seem to do more harm than good which is what brings me here.
Amanda: problems with fat digestion are often caused by a sluggish gall bladder and/or low stomach acid. The fats in the fish and the olive oil wouldn’t be responsible for hypoglycemia, mood swings or weight gain. Try supplementing with ox bile and betaine HCL with pepsin right at the start of meals. That should help.
RE: Fat Maldigestion and Fat Malabsorption
Chris: Hi, I’m a loyal fan since my Hashi dx in Nov, 2013. I’m currently 47, post-menopausal due to early-menopause at age 41 (likely dt an undiagnosed Hashis). After carefully applying much of the online and book advice from the Paleo & Hashi online communities, I have lost 30lbs (not an easy feat for a post-menopausal woman) and cut my TgAb in half from “9” to “4.5”. Your website/articles/book/store/radio show have been a constant companion during this journey, for which I am very grateful, thank you!
I got the results of my GI Effects stool test weeks ago (collected on 2/20/14) and it indicated that “Total SCFAs”, and Lactobacillus spp. was “low”. It also indicated that I don’t handle fats very well: High Triglycerides means “fat maldigestion”, High LCFAs means “fat malabsorption due to pancreatic, biliary insufficiency, or acute bacterial infection that produces intestinal cell destruction.” and High Total Fat “usually signals malabsorption (fat)”. Given that my pancreatic elastase 1 was great: “>500” and that the test showed no parasites, no yeast/fungi, no opportunistic bacteria, and no out of range “predominant bacteria” (except for the low lactobacillus spp.”, I assumed that my fat digestion/absorption problems were related to “biliary insufficiency”, some kind of gallbladder problem as you referenced in your above reply: “sluggish gallbladder”. Since I don’t have pain (although I’ve had GB-like URQ pain in my 20s and 30s from yo-yo dieting) and I don’t have steatorrhea, my doc and I both agreed it didn’t seem necessary to obtain a GB ultrasound. I was already taking Betaine HCL with pepsin prior to the study (Izabella Wentz, Thyroid Pharmacist recommended it in her book; of course, you recommend it too)
So, I started taking digestive enzymes (with ox bile) since I did not want to cut back too drastically on my added oils (now, about 3 Tbs coconut oil/day and 1-2tsp/olive oil). My diet is already very strict: AI Paelo approach (I also don’t eat fruit, right now, but I did add low-fructose starchy vegetables to my diet – about 30-40g/day – when stool results showed “low SCFAs”). So, I was probably consuming 5-6T of coconut oil at the time of the test. I also was not used to consuming high amounts of animal fats prior to my Hashi dx with subsequent diet changes. I’ve been taking the ox bile supplement “with meals” per the bottle recommendations.
So, HERE’s MY QUESTIONs:
1) Would you consider writing one of your famous articles on “fat digestion/fat absorption”? It seems that fat intake changes greatly when switching to Paleo along with the protein changes.
2) When is the best time (before, during, after meals) to take an ox bile supplement?
3) How soon do you recommend repeating a GI Stool test? Or, is there another, maybe less expensive, way to determine how one’s body is digesting/absorbing fats?
4) Is there a better, different ox bile supplement that you recommend?
5) Are there any other supplements that you recommend?
6) Do you recommend limiting fats until one’s fat absorption changes? And, by how much?
7) Since the stool test, I’ve noticed that sometimes, I do have undigested food in my stools, most recently, unsweetened coconut shreds. So, “undigested food in stools” is another symptom of fat malabsorption”, is that a reliable indicator for self-monitoring? If you don’t have undigested food in your stools, no floating stools, no oil, etc, then fat absorption can be assumed to be doing okay?
8) At what point is “fat malabsorption” something that requires further testing, like abdominal ultrasounds or small bowel biopsy or a hydrogen breath test to r/o small intestinal bacterial overgrowth, for example?
Or a pancreatic enzyme would be helpful. (and less concerning than HCL)
How long does it usually take for some relief to start when using HCL and eating low-carb? My symptoms are a constant burning in my upper esophagus and throat. Will it take time for that to go away as my body heals, or should it go away as immediately?
Everyone’s different. For some relief is relatively immediate, others it takes a bit of time. Either way, it’s worth it!
I have the same symptoms, feeling of acid in my throat .
Dr Do you think that the HCL will work for met?
I had an endoscopy 2 years ago, the gastro said I have a small hiatal hernia,, but at that time, I only experience pain in my stomach and feeling of a lump in my throat, but I took Prilosec OTC and in time and relaxing it went away.
Now, I have had a lot of very stressful circumstances, and the acid before never went to my throat, and now it does!
Can you please help me? with any suggestions?
Thank you!