

This is the second article in a series on heartburn and GERD. If you haven’t read the first one, I’d suggest doing that first.
The idea that heartburn is caused by too much stomach acid is still popular in the media and the public. But as Daniel pointed out in the comments section of the last post, anyone familiar with the scientific literature could tell you that heartburn and GERD are not considered to be diseases of excess stomach acid.
Instead, the prevailing scientific theory is that GERD is caused by a dysfunction of the muscular valve (sphincter) that separates the lower end of the esophagus and the stomach. This is known as the lower esophageal valve, or LES. The LES normally opens wide to permit swallowed food and liquids to pass easily into the stomach. Except for belching, this is the only time the LES should open.
Here’s the key point. It doesn’t matter how much acid there is in the stomach. Even a small amount can cause serious damage. Unlike the stomach, the lining of the esophagus has no protection against acid.
Free eBook
Learn More about Heartburn and GERD
Download this free eBook to discover the little-known causes of heartburn and GERD, and find out how to get rid of the problem forever.
"*" indicates required fields
I hate spam, too. Your email is safe with me. By signing up, you agree to our privacy policy.
We’ve Been Asking the Wrong Question
In an editorial published in the journal Gastroenterology, the author remarked: (1)
Treating gastroesophageal reflux disease with profound acid inhibition will never be ideal because acid secretion is not the primary underlying defect.
I couldn’t agree more. For decades the medical establishment has been directing its attention at how to reduce stomach acid secretion in people suffering from heartburn and GERD, even though it’s well-known that these conditions are not caused by excess stomach acid. Instead, the question researchers should have been asking is, “what is causing the LES to malfunction?” Since it is universally agreed upon that this is the underlying mechanism producing the symptoms of GERD, wouldn’t it make sense to focus our efforts here? That’s exactly what we’re going to do in this article.
GERD Is Caused by Increased Intra-Abdominal Pressure
It is well accepted in the literature that GERD is caused by an increase in intra-abdominal pressure (IAP).
For example, several studies have indicated an association between obesity and GERD, and one paper in Gastroenterology concluded that increased intra-abdominal pressure was the causative mechanism. (2, 3) But while I agree that all of the currently accepted factors play a role, I do not think they are the primary causes of the increased IAP seen in GERD.
The Two Primary Causes of Increased Intra-Abdominal Pressure
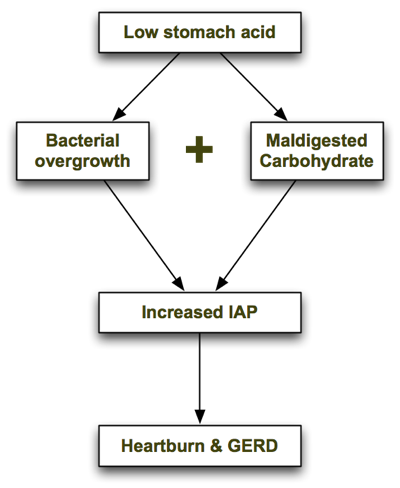
In his excellent book, Heartburn Cured, microbiologist Dr. Norm Robillard argues that carbohydrate malabsorption leads to bacterial overgrowth, resulting in IAP which drives reflux. Dr. Robillard makes a strong case that carbohydrate malabsorption plays a significant role in IAP, and I agree. But as I researched this issue I couldn’t help asking: what might be causing the carbohydrate malabsorption in the first place, and are there any other causes of bacterial overgrowth that may precede carbohydrate malabsorption? I believe the one answer to both of those questions is low stomach acid. Low stomach acid can contribute to both bacterial overgrowth (independently of carbohydrate intake) and carbohydrate malabsorption, as I describe below. In a nutshell, the process looks like this: Let’s look at each step in turn.
1. Low Stomach Acid Causes Bacterial Overgrowth
As I explain in the next article, one of the chief roles of stomach acid is to inhibit bacterial overgrowth. At a pH of 3 or less (the normal pH of the stomach), most bacteria can’t survive for more than 15 minutes. But when stomach acid is insufficient and the pH of the stomach rises above 5, bacteria begin to thrive. The gastrin knockout mouse, which is incapable of producing stomach acid, suffers from bacterial overgrowth—as well as inflammation, damage and precancerous polyps in its intestines. (4) It is also well documented that acid-suppressing drugs promote bacterial overgrowth. Long-term use of Prilosec, one of the most potent acid suppressing drugs, reduces the secretion of hydrochloric acid (HCL) in the stomach to near zero. In one trial, 30 people with GERD were treated with a high dose of Prilosec (40g/day) for at least 3 months. (5) Eleven of the 30 Prilosec-treated people had developed significant bacterial overgrowth, compared with only one of the 10 people in the control group.
2. Low Stomach Acid Causes Maldigestion of Carbohydrates
Stomach acid (HCL) supports the digestion and absorption of carbohydrates by stimulating the release of pancreatic enzymes into the small intestine. If the pH of the stomach is too high (due to insufficient stomach acid), the pancreatic enzymes will not be secreted and the carbohydrates will not be broken down properly.
Like what you’re reading? Get my free newsletter, recipes, eBooks, product recommendations, and more!
Bacterial Overgrowth + Maldigested Carbohydrates = GAS!
In Hearburn Cured, Dr. Robillard points out that though microbes are able to metabolize proteins and even fats, their preferred energy source is carbohydrate. The fermentation of carbohydrates that haven’t been digested properly produces gas. The resulting gas increases intra-abdominal pressure, which is the driving force behind acid reflux and GERD. From Dr. Robillard’s book:
According to Suarez and Levitt (17), 30 g of carbohydrate that escapes absorption in a day could produce more than 10,000 mL (ten liters) of hydrogen gas. That is a huge amount of gas!
When stomach acid is sufficient and carbohydrates are consumed in moderation, they are properly broken down into glucose and rapidly absorbed in the small intestine before they can be fermented by microbes. However, if stomach acid is insufficient and/or carbohydrates are consumed in excess, some of the carbs will escape absorption and become available for intestinal microbes to ferment.
Other Supporting Evidence
Dr. Robillard also argues that if gas produced by microbial fermentation of carbohydrates causes acid reflux, we might expect that reflux could be treated by either:
- Reducing bacterial overgrowth, or
- Reducing carbohydrate intake.
He points to two studies which demonstrate this. In a study by Pehl, administration of erythromycin (an antibiotic) significantly decreased esophageal reflux. (6)
In another study by Pennathur, erythromycin strengthened the defective lower esophageal sphincter in patients with acid reflux. (7) To my knowledge, there have only been two small trials performed to test the effects of carbohydrate restriction on GERD. Both had positive results. A small case series showed a significant, almost immediate resolution of GERD symptoms in obese individuals initiating a very-low-carb diet. (8) A more recent study found that a very low-carb diet decreased distal esophagus acid exposure and improved the symptoms of GERD. (9) Perhaps most importantly, the magnitude of the improvement was similar to what has been reported with treatment with proton-pump inhibitors (acid suppressing drugs).
Some researchers now believe that Irritable Bowel Syndrome (IBS) is caused by small intestinal bacterial overgrowth (SIBO). (10) A study performed at the GI Motility Center in Los Angeles in 2002 found that 71 percent of GERD patients tested positive for IBS—double the percentage seen in non-GERD patients being examined. (11) The high prevalence of IBS in GERD patients combined with the recognition that bacterial overgrowth causes IBS is yet another line of evidence suggesting that bacterial overgrowth is also a causative factor in GERD.
Final Comments
To summarize, low stomach acid contributes to bacterial overgrowth in the bowel which in turn can lead to carbohydrate malabsorption (due to decreased pancreatic enzyme secretion). Malabsorption of carbohydrates, as Dr. Robillard has pointed out, increases intra-abdominal pressure and causes GERD.
Where Dr. Robillard and I differ is that I believe low stomach acid is the primary problem with GERD, with carbohydrate malabsorption playing a secondary role. I do think that improper digestion of proteins can, in fact, lead to GERD, whereas Dr. Robillard states in his book that putrefaction of proteins is more likely to cause flatulence. This may be so in most cases, but I’ve seen several patients in my practice on very-low-carbohydrate diets who still experience heartburn, which improves upon restoring proper stomach acid secretion (which we covered in another article in this series). In the Part III of the series I discuss the connection between GERD and H. pylori, and further evidence supporting the theory that GERD is caused by bacterial overgrowth. Read on!
Better supplementation. Fewer supplements.
Close the nutrient gap to feel and perform your best.
A daily stack of supplements designed to meet your most critical needs.

I get very bad gas and reflux in morning. What is weird is I was so fed up with nothing working I drank a few beers to burp the gas out. Was difficult at first to swallow it but It worked like a charm, and every time I drank beer it went away and i became regular again instead of constipated all the time. What do you think that is from? I havent drank any beer for about a week, figured not a good long term plan haha. I have only had this bad gas/reflux 2 weeks and it is unbearable. Just purchased digestive enzymes, hci and apple cider vinegar. Going to give the digestive stuff a try but if it doesnt work I will go right back to the beer (i can’t handle how bad it gets) until the Doc figures it out, I think it is a bacteria. Tuesday hopefully it will be diagnosed correctly
Chris
Nice summary of the current research (2 years after your posting)! Provocative way of looking at GERD. I wanted to clarify one point in your article: the studies on erythromycin improving GERD symptoms you cited were pointing to the immediate improvement of symptoms following IV administration of e-mycin pre-meals. They were postulating the prokinetic and direct effects on LES tone that e-mycin has, rather than the antibiotic treating SIBO, per se.
That said, antibiotics are indeed used for treating SIBO, but the symptoms usually take longer than the above mentioned studies report for resolution. Here is an article talking about e-mycin (and antibiotics in general) being used for SIBO/IBS:
https://www.ncbi.nlm.nih.gov/pubmed/20574504
https://www.ncbi.nlm.nih.gov/pubmed/2028847
Thanks again!
I am grateful that you published an extensive & thorough discussion about acid reflux and GERD. It’s very enlightening and informative.
I was diagnosed of acid reflux 6 years ago and I’m still suffering from it until now. It frequently occurs at the middle of the night. When it attacks I also have heart palpitation. What is the relation of reflux to palpitation?
I hope you could help me with this.
Thank you very much. God bless.
I stumbled across your website today and it’s really great. I ended up here through an extensive Google search trying to figure out why I am extremely bloated, constipated (I go maybe once a day or every other day but I feel like it’s not all getting out–or maybe I’m filled with gas, although I’m not able to pass it often), and never really feel hungry. When it’s time to eat I already feel full within a bite or two!
I think through your info the lightbulb is starting to go on…several years ago I had a couple episodes of food regurgitating back into my throat, lots of burping, and a burning sensation at the top of my chest. Never having experienced that before I went to the doctor and they sent me to a specialist for an endoscopy. I was in my late twenties at the time and 40 pounds heavier–I ate horribly and hardly ever had whole fruits and veggies.
They told me I had a mild case of GERD, said to avoid mint, chocolate, caffeine, and fatty foods, and prescribed Aciphex which I took for about 3 years. Now that I am wiser and trying to eat well, I wonder why they just didn’t send me to a nutritionist and make changes there! Three years into taking the Aciphex, I started having noticeable lower right abdominal discomfort. I had a hernia ruled out at the time. So I stopped taking the Aciphex against the advice of the specialist who told me to also take Citrucel for my ab pain, which he thought was just constipation. I felt sick taking the Citrucel so I stopped.
Between then and now, I discovered I had a wheat allergy—possibly Celiac—and they recommended another endoscopy. I said I didn’t want another one so I just started eating as if I were Celiac and as a result I’ve felt SO good and dropped 40 pounds. However, for the past few months the right abdominal discomfort is back and sometimes almost painful, but it comes and goes and so I think it’s intestinal.
Sorry for the life report, but after all that—do you think that even after all this time I might have hypochlorhydria and could benefit from the HCL? It’s been especially worse since in the last few weeks I have been eating more fiber to ease what I think is the constipation because of the ab pain and also lower back pain on the right side (not the spine, but muscle area). Once I stopped the Aciphex, added more veggies and fruit, stopped the wheat and stayed away from the mint, chocolate, caffeine, and fatty foods I have not had a SINGLE case of acid reflux symptoms in all this time. I just feel so bloated, gassy, and full but can’t seem to find relief. I tried one of those Activia yogurts today and two slices worth of lemon juice…it felt a little better…but??? Would wine at dinner help? Or grapes?
Thank you, Chris!
Great article. I had just forwarded it to my husband to read since he is the one who has this occasional heartburn, a couple days a week.
I do have a question about this. His heartburn is kind of predictable, it depends on what he eats first thing in the morning… If he drinks tea with honey, he’ll get one and it’ll last all day long. Or a bowl of soup for example, basically almost any liquid meal/drink will cause it. Except coffee though, maybe because he has that cup after his hearty breakfast of eggs. Why would his body have a heartburn after tea or soup but not after coffee or any other ‘heavy’ food. He is overweight and I always thought it was because of the pressure as explained in this article. OH and he loves his carbs. I would love to hear your thoughts on this! 😉
Thank you! I’m not new to all this info but am new to your site 🙂
With the honey I would have said that it’s feeding the bad gut bacteria that are contributing to the gas and pressure against the LES, but that doesn’t make sense with soup. Perhaps he’s sensitive to the free glutamate in the soup broth and the tanins in the tea.
Please let me know where I can find out more information and more articles from Chris Kresser.
Is it safe to take HCL when pregnant..I had amazing results before I got pregnant, but am reading a lot about questioning the safety when pregnant..I am taking 150 mg tablets 3 x’s per day..thanks!
Hello,
I am having frequent sore throats.I think this might be because of the acid refux.Please suggest what to do?
Very elegant demonstration.
Just to understand clearly : the increase in intra-abdominal pressure occurs because of too much H2 in the gut, which then compresses the stomach, which pushes acid into the oesophagus. Is that correct?
WOW
I am profoundly grateful and impressed by your article. I have suffered from a “weak” LAS for years and this is the first article I have read that emanates deep study, good sense and intelligence.. Congrats!
I’ve been taking 20 mg of Omeprazol daily for about 10 years (I’m 40 now) and I really want to stop taking it. I tested negative for Pilory and my concern is if I stop taking Omeprazole, even if I don’t show gerd symptoms, I’ll have a high risk of cancer of the esophagus because of the sphincter. I know this med causes side effects, specially with bones (osteoporosis?), so shall I risk going off it?
Thanks for your article!!!!
I am kind of in the same boat. I have suffered from gerd or “weak” LAS for so many years. I feel like mine was brought on by diet and heavy alcohol consumption and then exacerbated by stress. Every time I went to the doctor, I was prescribed a different medicine. I have been on Omeprazol and other antacids for over 10 years. I am so mad at the Medical community, because the worse my condition got, the more antacids I took. Recently I went off of them and have been taking pribiotics. My problem is always when I lay down at night. Every morning I wake up with acidic taste in my mouth and there are certain foods that make me have severe gerd for days including garlic and cloves. I just wonder what it is about garlic that makes me have really bad acid reflux. Also I would love a sample diet or list of foods that we should eat to help combat the side effects of taking antacids for years and that can take away the bad bacteria that we have built up.
Hi
I did have the acid test and i do have low acid but when i take hcl it makes the problem worse! I have small bowel bacterial overgrowth.
Why would i feel worse?
So glad I found your website! I have been on Fluticasone Propionate Nasal Spray, Symbicort inhaler and then had a Kenalog Injection (all corticorteriods Triaminolone Acetonide) for allergies. Now do I have stomach and intestine problems. Gas, bloating, constipation, stomach gurgles bad (especially at night) sometimes indigestion. I feel like a wreck! What should I do??Thanks!
Chris, do you feel that paleo diet is best for someone with polycystic kidney disease? Eating paleo does help my reflux and does raise my stomach acid, but eating low protein alkaline diet seems better for my kidneys. I’m really confused. Thanks for your input!
I had problems with daily acid reflux for more than 15 years, until a few years ago when I was diagnosed with hiatal hernia…My doctor was “assuring” me that there is very good medicine for this(proton pump inhibitors ) that I will have to take all my life. I didn’t really accepted that a physiological deformation can’t be fixed, so I started to do some googling… After I tried a few things, including abdominal massage and some speciffic physical exercises the most effective way to reduce my acid reflux was by losing weight! I lost weight using a low carb diet inspired by the Atkins diet, but not that brutal…I’m basicaly cured from my chronic acid reflux and free from any medicine. I’m really glad that I discovered this website and this article and now I’m making sens of how negatively refined carbs affects digestion. I just wish that more people with similar problems would find out about this “cure”…! Thanks!
i’m a female age 30 years and have never had a good stomach, recentley i have had a very difficult time, that started with an Iron Deficiency and weight loss.I was put on Iron theapy but was malabsorbing so was referred to a gastro and had a gastroscopy and colonoscopy to see what was happening, the gastroscopy showed that i had 50+ ulcers in my stomach !!!! I was put on 40mg of Nexium a day to heal them, the gastroenterologist was astounded i had no gastro symptoms of the ulcers at all. I have been fine for just over a year, i’ve put weight and started to feel more healthy, untill just before Christmas when i started with reflux, i thought i had a throat infection to start with because my throat was sore and i had a horrid taste in my mouth, my GP tried various combinations of things, none of which seemed to help. Over the course of Christmas i came to the conclusion it may be caused by lactose intolerance so i canged my diet and it went well for a week or so and then started up again although the lactose free diet seems to have cured the bloating.I feel constantly sick and its really starting to get me down. I thought i must have had loads of acid otherwise what caused all the ulcers, because they still dont know, i was tested for zollinger ellisons and it wasnt that. Any thoughts welcome
Hi Chris,
I’m a mom of a one year old that has had suspected reflux and possible milk protein intolerence since she was 2-3 months old. She’s been on zantac and now Nexium (currently 15mg in the morning). I HATE that she has been on these meds. She has had constipation problems and still has suspected reflux symptoms on and off. She can’t talk so it’s hard to ever really know what’s going on but she has never been a good sleeper and is always being woken up in the middle of the night by something and then often can’t return to sleep. After reading all of your articles, I’m more determined than ever to get her off of the meds. Any suggesstions for a 1 year old on weaning and how to manage the reflux symptoms she may still have from an underdeveloped anatomy?
Hello Chris, thank you so much for these article series — they really are a life saver for me!
I do have two questions though:
1) What do you recommend to eat for breakfast? I seem to have zero stomach acid early in the day and I find that paleo foods, in fact any meat/fish, first thing in the morning does not digest at all.
2) This question is related to the first one. I am breastfeeding right now and was told I cannot take HCl by my doctor as well as my lactation consultant. I have tried ACV, lemon juice, fennel seed, raw sauerkraut, probiotics, DigestGold, but I can’t seem to raise my stomach acid sufficiently. I have taken HCl a couple of times and it made me feel fantastic, but since I can’t take it for now, is there anything else you can suggest? Fats do seem to help a bit (coconut oil, butter, bacon grease), but I don’t always have access to these foods at every meal, but breakfast is the most problematic. Please help!
Thanks!
Jean
Great article, I really enjoyed it! My husband experienced terrible GERD for his entire adult life until he started taking Prilosec. It seemed like magic. But what was truly magical is that he didn’t “need” Prilosec once he switched to a low-carb, paleo diet.
I am 7 1/2 months pregnant and suddenly have terrible GERD 24/7. I follow the diet in the Healthy Baby Code, consuming lots of raw milk, egg yolks, pastured meats, etc. and avoiding food toxins. It is no mystery what is causing pressure in my abdomen, but I was wondering if you have any suggestions on remedies that are safe during pregnancy. I do not have any gas or other digestive issues, just GERD. I’ve thought about trying the apple cider vinegar but I want to confirm that it is safe during pregnancy. Any tips would be greatly appreciated! Also, it might be a great addition to the reference material in the Healthy Baby Code. 🙂
Hi, Chris thank you very much!
I’ve suffered from GERD for years without relieve from conventional drugs (PPI & antacids). From your articles I am able to put almost all puzzle pieces about GERD’s causes, symptoms, & treatment in its place after years of researching.
But one thing still isn’t resolved. It’s hunger sensation, which constantly afflict many GERD sufferers including me .
Is it caused by excess gas in guts and stomach? Thanks.
Hi Chris,
41 year old male. No major health issues. I have never had any issues with heartburn until last Monday, November 28, 2011. Shortly after dinner I noticed I had a little heartburn afterwards. I went to gym 3 hours later and still had the heart burn. Now, 5 days later I still have it. Last night, in the evening the heart burn went completely away until I awoke today when it came back after dinner. Can acid reflux come on that quick? My stomach is sour. Looser than normal stool. And occasional burps. Before I found this site I was thinking I might have some type of stomach bacteria or virus? My father has a hiatus hernia which he has had for years. And my fathers sister has the same condition. I was a heavy Red Bull drinker for a year. But I stopped drinking them about 3 months ago. Not sure if that could be related or not.
Chris I had one other though. A long shot but I thought I would ask. My nephew recently had mono. And I was reading how Esophagitis can be caused from Herpes. Now mono is in the Herpes family, correct? Is it possible I contracted a strain of the mono virus from my nephew which is not attacking my Esophagus?
I don’t have any food coming back up. No vomiting or nauseousness. No weird tastes in my mouth. Just heartburn sensations, sour stomach occasionally. And sometimes a sore throat when I eat.