

This is the second article in a series on heartburn and GERD. If you haven’t read the first one, I’d suggest doing that first.
The idea that heartburn is caused by too much stomach acid is still popular in the media and the public. But as Daniel pointed out in the comments section of the last post, anyone familiar with the scientific literature could tell you that heartburn and GERD are not considered to be diseases of excess stomach acid.
Instead, the prevailing scientific theory is that GERD is caused by a dysfunction of the muscular valve (sphincter) that separates the lower end of the esophagus and the stomach. This is known as the lower esophageal valve, or LES. The LES normally opens wide to permit swallowed food and liquids to pass easily into the stomach. Except for belching, this is the only time the LES should open.
Here’s the key point. It doesn’t matter how much acid there is in the stomach. Even a small amount can cause serious damage. Unlike the stomach, the lining of the esophagus has no protection against acid.
Free eBook
Learn More about Heartburn and GERD
Download this free eBook to discover the little-known causes of heartburn and GERD, and find out how to get rid of the problem forever.
"*" indicates required fields
I hate spam, too. Your email is safe with me. By signing up, you agree to our privacy policy.
We’ve Been Asking the Wrong Question
In an editorial published in the journal Gastroenterology, the author remarked: (1)
Treating gastroesophageal reflux disease with profound acid inhibition will never be ideal because acid secretion is not the primary underlying defect.
I couldn’t agree more. For decades the medical establishment has been directing its attention at how to reduce stomach acid secretion in people suffering from heartburn and GERD, even though it’s well-known that these conditions are not caused by excess stomach acid. Instead, the question researchers should have been asking is, “what is causing the LES to malfunction?” Since it is universally agreed upon that this is the underlying mechanism producing the symptoms of GERD, wouldn’t it make sense to focus our efforts here? That’s exactly what we’re going to do in this article.
GERD Is Caused by Increased Intra-Abdominal Pressure
It is well accepted in the literature that GERD is caused by an increase in intra-abdominal pressure (IAP).
For example, several studies have indicated an association between obesity and GERD, and one paper in Gastroenterology concluded that increased intra-abdominal pressure was the causative mechanism. (2, 3) But while I agree that all of the currently accepted factors play a role, I do not think they are the primary causes of the increased IAP seen in GERD.
The Two Primary Causes of Increased Intra-Abdominal Pressure
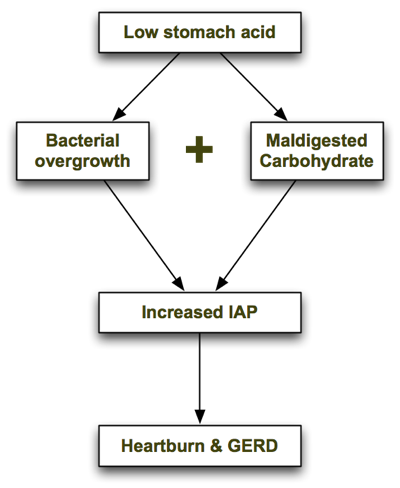
In his excellent book, Heartburn Cured, microbiologist Dr. Norm Robillard argues that carbohydrate malabsorption leads to bacterial overgrowth, resulting in IAP which drives reflux. Dr. Robillard makes a strong case that carbohydrate malabsorption plays a significant role in IAP, and I agree. But as I researched this issue I couldn’t help asking: what might be causing the carbohydrate malabsorption in the first place, and are there any other causes of bacterial overgrowth that may precede carbohydrate malabsorption? I believe the one answer to both of those questions is low stomach acid. Low stomach acid can contribute to both bacterial overgrowth (independently of carbohydrate intake) and carbohydrate malabsorption, as I describe below. In a nutshell, the process looks like this: Let’s look at each step in turn.
1. Low Stomach Acid Causes Bacterial Overgrowth
As I explain in the next article, one of the chief roles of stomach acid is to inhibit bacterial overgrowth. At a pH of 3 or less (the normal pH of the stomach), most bacteria can’t survive for more than 15 minutes. But when stomach acid is insufficient and the pH of the stomach rises above 5, bacteria begin to thrive. The gastrin knockout mouse, which is incapable of producing stomach acid, suffers from bacterial overgrowth—as well as inflammation, damage and precancerous polyps in its intestines. (4) It is also well documented that acid-suppressing drugs promote bacterial overgrowth. Long-term use of Prilosec, one of the most potent acid suppressing drugs, reduces the secretion of hydrochloric acid (HCL) in the stomach to near zero. In one trial, 30 people with GERD were treated with a high dose of Prilosec (40g/day) for at least 3 months. (5) Eleven of the 30 Prilosec-treated people had developed significant bacterial overgrowth, compared with only one of the 10 people in the control group.
2. Low Stomach Acid Causes Maldigestion of Carbohydrates
Stomach acid (HCL) supports the digestion and absorption of carbohydrates by stimulating the release of pancreatic enzymes into the small intestine. If the pH of the stomach is too high (due to insufficient stomach acid), the pancreatic enzymes will not be secreted and the carbohydrates will not be broken down properly.
Like what you’re reading? Get my free newsletter, recipes, eBooks, product recommendations, and more!
Bacterial Overgrowth + Maldigested Carbohydrates = GAS!
In Hearburn Cured, Dr. Robillard points out that though microbes are able to metabolize proteins and even fats, their preferred energy source is carbohydrate. The fermentation of carbohydrates that haven’t been digested properly produces gas. The resulting gas increases intra-abdominal pressure, which is the driving force behind acid reflux and GERD. From Dr. Robillard’s book:
According to Suarez and Levitt (17), 30 g of carbohydrate that escapes absorption in a day could produce more than 10,000 mL (ten liters) of hydrogen gas. That is a huge amount of gas!
When stomach acid is sufficient and carbohydrates are consumed in moderation, they are properly broken down into glucose and rapidly absorbed in the small intestine before they can be fermented by microbes. However, if stomach acid is insufficient and/or carbohydrates are consumed in excess, some of the carbs will escape absorption and become available for intestinal microbes to ferment.
Other Supporting Evidence
Dr. Robillard also argues that if gas produced by microbial fermentation of carbohydrates causes acid reflux, we might expect that reflux could be treated by either:
- Reducing bacterial overgrowth, or
- Reducing carbohydrate intake.
He points to two studies which demonstrate this. In a study by Pehl, administration of erythromycin (an antibiotic) significantly decreased esophageal reflux. (6)
In another study by Pennathur, erythromycin strengthened the defective lower esophageal sphincter in patients with acid reflux. (7) To my knowledge, there have only been two small trials performed to test the effects of carbohydrate restriction on GERD. Both had positive results. A small case series showed a significant, almost immediate resolution of GERD symptoms in obese individuals initiating a very-low-carb diet. (8) A more recent study found that a very low-carb diet decreased distal esophagus acid exposure and improved the symptoms of GERD. (9) Perhaps most importantly, the magnitude of the improvement was similar to what has been reported with treatment with proton-pump inhibitors (acid suppressing drugs).
Some researchers now believe that Irritable Bowel Syndrome (IBS) is caused by small intestinal bacterial overgrowth (SIBO). (10) A study performed at the GI Motility Center in Los Angeles in 2002 found that 71 percent of GERD patients tested positive for IBS—double the percentage seen in non-GERD patients being examined. (11) The high prevalence of IBS in GERD patients combined with the recognition that bacterial overgrowth causes IBS is yet another line of evidence suggesting that bacterial overgrowth is also a causative factor in GERD.
Final Comments
To summarize, low stomach acid contributes to bacterial overgrowth in the bowel which in turn can lead to carbohydrate malabsorption (due to decreased pancreatic enzyme secretion). Malabsorption of carbohydrates, as Dr. Robillard has pointed out, increases intra-abdominal pressure and causes GERD.
Where Dr. Robillard and I differ is that I believe low stomach acid is the primary problem with GERD, with carbohydrate malabsorption playing a secondary role. I do think that improper digestion of proteins can, in fact, lead to GERD, whereas Dr. Robillard states in his book that putrefaction of proteins is more likely to cause flatulence. This may be so in most cases, but I’ve seen several patients in my practice on very-low-carbohydrate diets who still experience heartburn, which improves upon restoring proper stomach acid secretion (which we covered in another article in this series). In the Part III of the series I discuss the connection between GERD and H. pylori, and further evidence supporting the theory that GERD is caused by bacterial overgrowth. Read on!
Better supplementation. Fewer supplements.
Close the nutrient gap to feel and perform your best.
A daily stack of supplements designed to meet your most critical needs.

I would like to know what you would recommend for someone who’s digestive system is underperforming (hypochlorhydria, enzyme insufficiency, constipation, suspected overgrowth), but who also has gastritis. HCL/enzymes improve my digestion greatly, but I can’t take HCL because of my damaged stomach lining which produces pain upon coming in contact with anything acidic. However, if I don’t take HCL, then I get gassy and constipated again. It’s a Catch-22: I need acid but can’t take ANY amount of it. Suggestions?
Erika,
I am not a health-care professional, but can speak to my own experience. Although I haven’t had an “official” diagnosis of gastritis, I have no doubt that my stomach is inflamed. I have recently started taking a supplement which includes l-glutamine with excellent results (Intestinew is the brand name). You can find lots of information if you just Google l-glutamine. Although l-glutamine has basically cleared up the chronic burning from heartburn — after 15+ years (YEAH!!!), because my stomach still isn’t functioning optimally, I sometimes still have to take Betaine HCL with Pepsin, but in much smaller quantities and far less frequently than I had to pre Intestinew. It feels like a miracle. Good luck! I hope you find some relief.
Hi Erika,
What dosage & how often for l glutamine? How long did it take to heal the lining?
What if I had gastritis a year ago and also suffer from gerd. Can I take HCL supplements or can that destry my stomach.
Is it possible that, “Gluten Intolerance” could be linked to low stomach acid?
As you stated in 2nd article, Low stomach acid doesn’t break down carbs and leads to bad bacterial overgrowth in the intestines. Gluten Intolerance is just undigested gluten proteins right? So if we increase the stomach acid to better help digestion of food before entering the small intestine, could it help to break down the gluten protein? I don’t know enough about either issue but it was just a thought.
If low stomach acid is the problem, then why do acidifying foods make heartburn worse? E.g. coffee, coca cola, etc… Doctors also recommend avoiding them, but the fact is that doing so actually helps.
I was given prilosec by a doctor because I came in with nausea and other symptoms that I now believe are symptoms of H pylori. Every time I went off prilosec the symptoms came back. Iv been on prilosec for 4 years. I recently got blood work done at a lab and found I had h pylori antibodies, but wasn’t prescribed antibiotics. I need to get off Prilosec and kill H pylori. Any help? I have no idea where to start.
im from philippines i need help,i have acid reflux for two months ive tried all ppi and visit two GI Doctors still im not cured.I fell bloated and i cant burp,if i force to burp,wet burps comes out and thats make trouble at my throat. How can i test my acid of my stomachl,im not familiar with the 200g HCL is it available in our country can u give me the specs so i can purchased the right one….
Hi, I am conflicted of two of your articles – this one concerning causes of GERD and the one on histimine-intolerance and am hoping you can send me along the path of better choice…
My Hx:
I am in my early-thirties, I have had three children (between miscarriages). Eight years ago (when I was drinking two coffees a day – I now drink weak espresso-based drinks drown in milk) I was diagnosed with acid reflux disease and put on a slew of PPI’s (only having success with Nexium) in addition to a nasal corticosteriod when my symptoms are most severe after experiences of severe dysphagia and a strangling sensation around my throat. I seldom feel the sensation of “heartburn” itself.
I’ve been for a barium swallow and gastroscopy all showing “mild reflux” but the symptoms kept reccurring to various degrees and to this day I anxiety continues to accompany my meals though the food – while sometimes slow to go down, no longer feels stuck. So eventually I was sent for a swallowing study. No one was “concerned” with the results as everything looks like it is “minor”.
Three years ago I went in for a lap. cholecystectomy and since then I have found myself to often have feelings of trapped air – which is expected as normal – but I also hear gurgling in my upper GI tract, which I’ve never experienced. Again, the Nexium (40mg) relieves my symptoms while I take it (a few weeks at a time until I start getting jittery-feeling, lightheaded, and experience heart-palpatations – maybe not because of the drug, and maybe just my hormones or low iron, which is also an endless battle for me as I don’t eat red meat…I did ask my doctor to run my Mg++ levels and they came back okay). I usually stay symptom-free for a couple of weeks after, but then I need to resume if only one pill every three days.
Aside from all this – which I initally believed to be separate until I read your other article on histimine that tied it together for me – in high school one day I began to experience intense itchiness upon jogging which I had never experienced before. This problem continues to plague me though I continue to try to be active – previously it seemed that in time as I would become more fit I could build up the length of time I could walk briskly or run before my skin began to crawl – eyeballs and beneath fingernails included – and felt incredible anxiety, though each time I revisit embarking upon an excise regime, my intervals of being able to endure the horrendous pruritis seem to become shorter and shorter. Obviously, this is making life extremely frustrating and no doctor I have seen has acknowledged my condition to be a medical concern and up until now I have chalked it up to “normal” mast cell degranulation and subsequent histimine release upon exercise in response to the demands for vasodilation during my activity (however reading that it could potentially lead to anaphylaxis terrifies me, especially when my doctor will not prescribe me an epi-injector since my problem isn’t apparently medically valid).
Needless to say, I am excited at the thought of this possibly being able to be remedied – or at least better-controlled – through diet! And on a side note, my youngest has severe allergies and there are several things she eats that she was tested for and supposedly not allergic to that cause her fingers and face to puff up…which leads me to wonder if this condition could be afflicting her too and perhaps she has inherited it from me…
All that being said, I’ve recently finished a 10-day course of erythromycin for a strep infection of my throat that did not respond to seven days of amoxicillan and am wondering if I might have a “clean slate” for intestinal flora!(?) I have been taking a probiotic of 2 billion active cells of 5 different bacterial cultures (all but one that you listed to be appropriate for following a low-histimine diet which was not listed at all) and consume greek yogurt (Liberte Organic) daily. I have not taken Nexium for four weeks and my symptoms are beginning their usual rebound so I’m leaning toward resuming them, unless there is a way I could fix it through diet but I am unsure of which diet path to go down – one discusses an increase in fermented foods while the other requires staying far, far away from those same items.
Based on my history, would you think that my GERD is linked to my histimine levels and I should follow the low-histimine diet in hopes to improve both conditions simultaneously? Or does it make more sense to just focus on trying to resolve the acid-reflux through your suggested diet and get away from the drugs and deal with the histimine levels at a later time and not engage in vigorous exercise in the interim?
Thank you in advance for your time and insight.
Hi Chris,
My 43 year old son has experienced decades of GERD. Despite a myriad of tests, he’s had to live with prescription medications, diet control and even bicarb swigs for much of his life. He tested negative for h.pylori.
Amazingly, he told me last night that a course of antibiotics for strep throat seems to have cured his stomach problems. “I can actually eat anything I want now!” These 2 drugs seem responsible:
500mg Cefprozil twice daily for 7 days
250mg Cefaclor thrice daily for 7 days
What do you think happened here? We are very happy but puzzled.
Thanks for your help!
Chris
Hi Chris,
Your article was so interesting. My 4 kids have all had GERD. We have also noticed that they don’t tolerate milk with lactose well or when I nursed them and drank milk, the GERD symptoms were much worse. Recently, my oldest son (8yrs) was diagnosed with fructose malabsorbtion so we have put him on the FODMAP diet. So no carbs, milk, ect. We’ve been pleased to see there have been less headaches, heartburn, and better focus in school. I’m guessing all our children have this as well. I had no idea the connection between the GERD, lactose, and fructose malabsorbtion, until your article. Is fructose malabsorbtion the same as carb malabsorbtion? I too, can not eat an apple without getting heartburn. Can you tell me why? And do my children need to stay off carbs/limit carbs the rest of their lives or only until their guts heal?
Hi Katie! This post is interesting to me. I have told my doctors that I don’t think I can process sugars and they look at me like I’m crazy. Can you share what type of doctor diagnosed your son with this? I would love to insist that my doctors test for this to see if it indeed is causing or contributing to my debilitating GERD.
Thanks!!
Kelly
Hi Chris…i have severe reflux. I tried probiotics which were 20 billion. .the brand was megafood megaflora and it majorly worsened my reflux. Why wouldthis be? Also, if Acv worsened my reflux, does that mean i dont have low stomach acid? Thanks!
Hello Chris,
After being on Prevacid for more than 10 years, the drug stopped working. Food started backing up into my throat and I was starting to have to double up on the meds for it to stop the heartburn. At one point in conversations with my MD, I asked him if he thought it could be that I didn’t have a gallbladder. “NO” was the response. Because the meds were no longer effective, my MD sent me to a specialist to see about fundoplication surgery. I had to come off the meds to do the testing, and that turned out to be a lucky thing.
For the past 18 months, I have had heartburn, but I have had the opportunity to look at what is really causing my problems. It’s been a huge amount of trial and error, but I’ve finally found the magic combination. Digestive enzymes with bile salt and about 1500 mg of Betaine HCL with my meals.
I seriously have not felt this good in a decade. Now that I have something that seems to be working, I’m going to check with a Naturopath to see what else I can do to help with my situation, though I’m hoping that I have it well in hand.
Just wanted to share all of this with you and your website since the information you have provided has been extremely helpful.
Best regards,
Sandy
My mother had GERD and was taking all the medication that goes with it, with no improvement. Like you mentioned, she said the sphincter wouldn’t work and close properly to protect her. Then she was accidentally cured overnight when she had a problem with her neck and took a muscle relaxant. The relaxant also fixed her sphincter, and she immediately had no more problems.
I’ve got a tricky one for ya. My (8yr) daughter has a genetic salt-wasting kidney disorder. She takes Potassium Chloride (liquid, 213mEq per day, this is not a typo!), Magnesium Gluconate, Sodium Chloride, Indomethacin (similar to Advil), and Amiloride (potassium sparing diruetic).
A few years ago she developed a duodenal ulcer with a granulation tissue mass which obstructed her and caused vomiting. We had to give her a gasterostomy-tube and feed her pediasure for several months while we took her off her Indomethacin (and therefore had to raise her potassium) to help her heal. That’s the short version of the story. She actually underwent an octriotide scan, CT scan, PET/CT scan, Gastric Emptying test, Barium swallow. pH probe studies (2). She is now on TWO 20mg Omaprozol pills per day and has breakthrough reflux all the time. She also has fructose malabsorption.
She’s on a very low dose of Indomethacin now. 8.3mg per day, split into 3 doses.
Any recommendations? The pH probe studies indicated that she had a very low pH in her stomach when she’d reflux. They tried her on prevacid and it didn’t have any effect. Only the Omaprozol helped. Is there anything else I can do to help her?
I have been suffering with acid reflux all 4 years of college and now recently ibs symptoms have come up. I have been takig Prevacid for all this time, and I have gotten multiple yeast infections and bacterial infections of the throat. I never would have thought to assosiate these with the Prevacid!! Do you have any advice on how I would wean myself off of the Prevacid. I have tried once before with bad results. I would love any help! Great article 🙂
Hi,
I have GERD and Barretts disease. I am scheduled for fundoplication surgery in 2 weeks. Been on protonix for about 5 years. Last 2 years have constant chest pain and spasms in esophogus. All tests came back normal for acid levels. I have no heartburn, gas or burping. One test showed too much acid when I am in upright position for being on protonix. I also have hiatal hernia. Would rather not have the surgery. Looking for any suggestions to try so I don’t need surgery.
Thank You,
Patty
Patty,
Have you read the book “Dropping Acid” by Dr. Jamie Koufman? He speaks to “Silent Reflux” as it sounds as though that is what you are experiencing.
Another good book is “Why Stomach Acid is Good for You” by Jonathon Wright, MD.
I was experiencing Silent Reflux, but when I started taking Digestive Enzymes and Betaine HCL, those symptoms went TOTALLY away.
Good luck!
Saw this the other day, it might help. Good luck.
https://www.drdavidwilliams.com/how-to-fix-hiatal-hernia-naturally
I’m just letting you know that i have had the Nissan surgery and i would not recommend it to anyone. It never helped with my reflux and i have been sick ever since. Everyday i search the net to desperately find answers, I have found none yet but i do know one thing i wish i would of never had the surgery.
When i went back to the dr he said that it was not a guarantee that this surgery would work. So he put me back on the meds that i was on before the surgery (they don’t tell you this till after the surgery) Its all about the money
Hey admin,
I was wondering if lack of stomach avoid can be caused by gall bladder removal?
Back story:
I was obese, about 135kg two years ago, my husband and I made the decision to become vegan (unrelated to weight). drastic change in diet, no more eating greasy takeaway and cakes etc, caused us to life weight very quickly. I lost about 30kg in the first 5 weeks. Then the gall stone attacks started. The doctors told me it was caused by the sudden weight loss and change from very high fat diet to low fat. I was also lucky enough to have a lot of small stones so I was constantly in pain. I was given oxy freely for three months and bumped to the top of the surgery queue. Surgery was successful no more pain. Recovery took a just over a week. Then I had what felt like another attack. Before I was diagnosed with stones they said it was gerd and I was started on ant acids, but as you can imagine they were unhelpful. The doctors kept increasing the strength of these and then they started looking for ulcers and that’s when they found the stones. So I had heaps of these medicines left over so when I got pain after the surgery I grabbed a pack and out of habit took a pill. This caused me the worst pain I have ever had and I was getting gall attacks a couple times a day so that’s saying something. Hubby rushed me to the and they have me some morphine. But this pain kept coming back. My flatmate who is naturopath gave me a bottle of hcl that she had ordered for her grandmother. WOW that changed my life. But I’m slowly learning about poor nutrient absorption and also that no one here has ever heard of this disorder! I have to order hcl of the internet because the pharmacies here have never heard of it. I always feel like an idiot asking for it, they always say like the acid? *facepalm*
So my question is should I be taking hcl with every meal? At yet moment I get pain around 2am but not every night, my food diary hasn’t revealed anything, and it’s been months now. So I just take some when I wake up with pain.
Is it possible to develop a tolerance to hcl? I’ve noticed lately I’ve had to take more and more before I get relief. What started with one pill had now before five. Which ties into the first question because it’s getting expensive.
Is it possible that a low carb diet will help, or low gluten? Previous to the surgery I had never had any stomach problems, never even heartburn or indigestion. So I’m mentality blaming this on the lack of a gall bladder and therefore I’m not sure if this is an allergy problem so to speak.
Any advice would be amazing. Sorry if you have already addressed this I read most of the comments above but not all. Also sorry for any poor grammar or spelling, it is 2am. 🙂
Thanks again
Kati
hi,
I have seen many specialist advisers here so i would like to ask you about the problem i m facing and which is getting serious day by day. I am suffering from GERD from almost an year, the problem started with the symptoms of nausea, appetite loss, bitter taste in mouth and some kind of smell related to mouth I didnt take it seriously at that time but when the condition was getting worst then I consult some gastroenterologist and went through sigmidoscopy and endoscopy, doctor diagnosed piles and acid reflux and gave me nexum capsule and motival tablet and he said the symptoms are because of stress and anxiety. I am taking those medicines from about 8 to 9 months beside this i tried homeopath medicines too but found nothing effective in both of them and i feel like there is nothing in this world which can reduce this reflux disease or give early relief to this problem. Nowadays my problem is getting worst and i am suffering from serious excessive gas problem and the food i ate comes back to the throat and cause burning effect to the throat and it happens through out the day daily. and i feel like gas is just stuck in upper opening of stomach and have to pull it to release it… plzzz help me to get rid of this or just tell me how to reduce it.. i have also restrict my diet from junk foods and too much spices… and one think i must add here i do smoking also and use some kind of weed…
Hello:
Over a year ago, I started on a low-carb (Atkins) diet, to control Type II Diabetes. An immediate (within days) and totally unexpected side effect was the complete disappearance of all symptoms of GERD. Still on the diet (and loving it) over a year later, not only is my blood sugar normal, but the GERD has never returned. Excess carbohydrate intake was the culprit–cut the carbs and the heartburn and GERD are gone.
Hi,
what are your thoughts about the stretta procedure to help with acid reflux? Also, when I jog, I can only go about five or ten minutes before my reflux seems to act up…any way I can prevent it?…..thanks