

In the last article we discussed the problems humans have converting omega-3 (n-3) fats from plant sources, such as flax seeds and walnuts, to the longer chain derivatives EPA and DHA. Since EPA and DHA (especially DHA) are responsible for the benefits omega-3 fats provide, and since EPA and DHA are only available in significant amounts in seafood, it follows that we should be consuming seafood on a regular basis.
But how much is enough? What does the research literature tell us about the levels of EPA and DHA needed to prevent disease and ensure proper physiological function?
I’m going to answer this question in detail in the next article. But before I do that, I need to make a crucial point: the question of how much omega-3 to eat depends in large part on how much omega-6 we eat.
The historical ratio of omega-6 to omega-3
Throughout 4-5 million years of hominid evolution, diets were abundant in seafood and other sources of omega-3 long chain fatty acids (EPA & DHA), but relatively low in omega-6 seed oils.
Anthropological research suggests that our hunter-gatherer ancestors consumed omega-6 and omega-3 fats in a ratio of roughly 1:1. It also indicates that both ancient and modern hunter-gatherers were free of the modern inflammatory diseases, like heart disease, cancer, and diabetes, that are the primary causes of death and morbidity today.
At the onset of the industrial revolution (about 140 years ago), there was a marked shift in the ratio of n-6 to n-3 fatty acids in the diet. Consumption of n-6 fats increased at the expense of n-3 fats. This change was due to both the advent of the modern vegetable oil industry and the increased use of cereal grains as feed for domestic livestock (which in turn altered the fatty acid profile of meat that humans consumed).
The following chart lists the omega-6 and omega-3 content of various vegetable oils and foods:
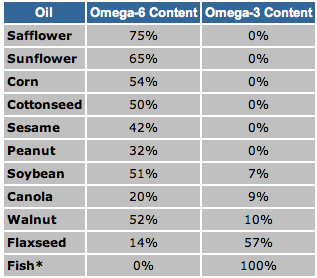
Vegetable oil consumption rose dramatically between the beginning and end of the 20th century, and this had an entirely predictable effect on the ratio of omega-6 to omega-3 fats in the American diet. Between 1935 and 1939, the ratio of n-6 to n-3 fatty acids was reported to be 8.4:1. From 1935 to 1985, this ratio increased to 10.3:1 (a 23% increase). Other calculations put the ratio as high as 12.4:1 in 1985. Today, estimates of the ratio range from an average of 10:1 to 20:1, with a ratio as high as 25:1 in some individuals.
In fact, Americans now get almost 20% of their calories from a single food source – soybean oil – with almost 9% of all calories from the omega-6 fat linoleic acid (LA) alone! (PDF)
This reveals that our average intake of n-6 fatty acids is between 10 and 25 times higher than evolutionary norms. The consequences of this dramatic shift cannot be overestimated.
Omega-6 competes with omega-3, and vice versa
As you may recall from the last article, n-6 and n-3 fatty acids compete for the same conversion enzymes. This means that the quantity of n-6 in the diet directly affects the conversion of n-3 ALA, found in plant foods, to long-chain n-3 EPA and DHA, which protect us from disease.
Several studies have shown that the biological availability and activity of n-6 fatty acids are inversely related to the concentration of of n-3 fatty acids in tissue. Studies have also shown that greater composition of EPA & DHA in membranes reduces the availability of AA for eicosanoid production. This is illustrated on the following graph, from a 1992 paper by Dr. William Landis:
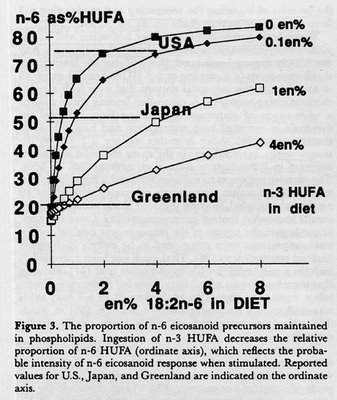
The graph shows the predicted concentration of n-6 in the tissue based on dietary intake of n-3. In the U.S. the average person’s tissue concentration of highly unsaturated n-6 fat is 75%.
Like what you’re reading? Get my free newsletter, recipes, eBooks, product recommendations, and more!
(Note: the ratio of omega-6 to omega-3 matters, but so does the total amount of each.)
In plain english, what this means is that the more omega-3 fat you eat, the less omega-6 will be available to the tissues to produce inflammation. Omega-6 is pro-inflammatory, while omega-3 is neutral. A diet with a lot of omega-6 and not much omega-3 will increase inflammation. A diet of a lot of omega-3 and not much omega-6 will reduce inflammation.
Big Pharma is well aware of the effect of n-6 on inflammation. In fact, the way over-the-counter and prescription NSAIDs (ibuprofen, aspirin, Celebres, etc.) work is by reducing the formation of inflammatory compounds derived from n-6 fatty acids. (The same effect could be achieved by simply limiting dietary intake of n-6, as we will discuss below, but of course the drug companies don’t want you to know that. Less profit for them.)
As we discussed in the previous article, conversion of the short-chain n-3 alpha-linolenic acid (ALA), found in plant foods like flax and walnut, to DHA is extremely poor in most people. Part of the reason for that is that diets high in n-6 LA inhibit conversion of ALA to DHA. For example, one study demonstrated that an increase of LA consumption from 15g/d to 30g/d decreases ALA to DHA conversion by 40%.
Death by vegetable oil
So what are the consequences to human health of an n-6:n-3 ratio that is up to 25 times higher than it should be?
The short answer is that elevated n-6 intakes are associated with an increase in all inflammatory diseases – which is to say virtually all diseases. The list includes (but isn’t limited to):
- cardiovascular disease
- type 2 diabetes
- obesity
- metabolic syndrome
- irritable bowel syndrome & inflammatory bowel disease
- macular degeneration
- rheumatoid arthritis
- asthma
- cancer
- psychiatric disorders
- autoimmune diseases
The relationship between intake n-6 fats and cardiovascular mortality is particularly striking. The following chart, from an article entitled Eicosanoids and Ischemic Heart Disease by Stephan Guyenet, clearly illustrates the correlation between a rising intake of n-6 and increased mortality from heart disease:
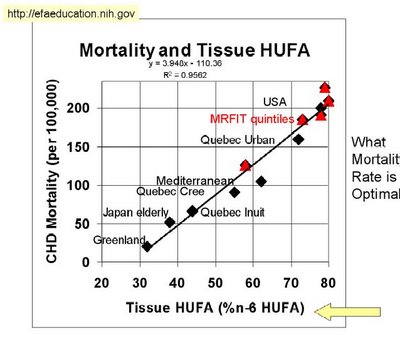
As you can see, the USA is right up there at the top with the highest intake of n-6 fat and the greatest risk of death from heart disease.
On the other hand, several clinical studies have shown that decreasing the n-6:n-3 ratio protects against chronic, degenerative diseases. One study showed that replacing corn oil with olive oil and canola oil to reach an n-6:n-3 ratio of 4:1 led to a 70% decrease in total mortality. That is no small difference.
Joseph Hibbeln, a researcher at the National Institute of Health (NIH) who has published several papers on n-3 and n-6 intakes, didn’t mince words when he commented on the rising intake of n-6 in a recent paper:
The increases in world LA consumption over the past century may be considered a very large uncontrolled experiment that may have contributed to increased societal burdens of aggression, depression and cardiovascular mortality.
And those are just the conditions we have the strongest evidence for. It’s likely that the increase in n-6 consumption has played an equally significant role in the rise of nearly every inflammatory disease. Since it is now known that inflammation is involved in nearly all diseases, including obesity and metabolic syndrome, it’s hard to overstate the negative effects of too much omega-6 fat.
In the next article, we’ll discuss three different methods for determining healthy intakes of n-3 that take background intake of n-6 into account.
Better supplementation. Fewer supplements.
Close the nutrient gap to feel and perform your best.
A daily stack of supplements designed to meet your most critical needs.

Sir, what is your take on Virgin coconut oil?
Can you tell me if the information given here is based on recent studies?By recent I mean within the last 12-24 months.Thank you
the asterisk signifies that the fatty acids contain DHA and EPA.
Question –
I eat what I call an “adapted Paleo” diet. (I have not read your book, but was very excited to see some of my beliefs validated on your blog and want to get to the book). The question is, when we eat this way, should we still take simply Omega-3 supplements? Or should we be moving toward a 3/6/9 supplement?
Are all omega-6 fatty acids pro-inflammatory?
During a discussion with a doctor( chemist) the following question came up. Why are all n-6 fatty acids “evil” if not all of them are actually pro-inflammatory. He suggested that the ration between aracidonic acid and EPA would be a better parameter than n-6/n-3.
What are your thoughts on that?
is it true that without taking omega-3 fatty acid can cause mental illness???
Yes Catherine!
Apparently the World Health Organization endorses an n-6 to n-3 ratio of 4:1. The researchers at https://www.pkprotocol.com also use this ratio in their treatment protocols, based on research by Yehuda, et. al. This ratio, of course, differs sharply from your target ratio. Chris, could you comment on this?
Why not test your fatty acid balance?
To see if your diet or Product works?
There is a dry blod sample test and I know how to get an extensive 30 pages test for free. You are welcome to connect with me on facebook to get mere Info.
Delighted to find a well-researched blog discussing omega 3 to 6 ratios, their background history, as well as modern sources of omega 3 fatty acids.
Although Chris acknowledges the overwhelming advantage of seafood over plant-sourced omega3, we are left with a serious dilemma– fish bear an ever greater toxic burden. To obtain adequate amounts of long-chain omega3 fatty acids, we are forced to eat not only toxins naturally present with fish, but industrial toxins like mercury, lead, PCBs and even chlordane.
Our alternative to seafood is endogenous conversion of plant-sourced, short-chain omega3 fatty acids. Since the human history does not involve ready access to seafood at all locations, humans survived on alternative sources of essential fatty acids. There may have been a native conversion ability to some degree, in particular populations. So, one potentially useful vein of research is the reason humans vary individually on their omega3 to 6 conversion ability– enzymes appropriate to the conversion are not evenly distributed in the population.
For most of us, lacking that conversion ability means we can obtain our DHA and EPA in complete safety from only molecularly-distilled fish oil. And to obtain a truly substantial amount of DHA and EFA by supplement not only requires ingestion of a considerable amount of oil, but is quite expensive.
Perhaps the better approach– hopefully made practical by research– is to identify and provide by oral supplement the enzymes needed to increase omega3 to 6 conversion efficiency with plant sources, such as flaxseed. At some later point, perhaps genetic engineering can splice the genes required to make the conversion “naturally”.
One of the hazards of editing late at night is to see what is not there. Here are two corrections–
“So, one potentially useful vein of research is to explore the reason humans vary individually on their omega3 short-chain to long-chain conversion ability”
and this
“is to identify and provide by oral supplement the enzymes needed to increase omega3 short-chain to long-chain conversion efficiency with plant sources, such as flaxseed. “
I agree wholly with Pone. This is truly a 2014, logical, rational and level headed thinking that we all should employ.
I hope 2014 brings with it common sense, ethical food and agriculture company’s as well as sound economic policy.
god speed to us all
George, when I have tried to make the same remarks about Omega-6 in public forums before, I get hit by an onslaught of hate mail from medical practitioners trying to defend the AHA’s many studies on Omega-6 lowering heart lipids.
The point the biochemists make in response is that the AHA studies with Omega-6 also use Omega-3, thus making causality to Omega-6 impossible to establish. A superb article summarizing both sides of this argument fairly is here:
https://www.asbmb.org/asbmbtoday/asbmbtoday_article.aspx?id=18365
If I already posted that link, sorry I forgot. 🙂
Even if there is only 40% chance the biochemists are right, why take the chance? I’m increasing my monounsaturated intake, lowering my saturated, and lowering to trace levels my Omega-6 (which is HARD HARD HARD to do given modern food practices).
I am a practicing MD. I have served as a clinical adviser to research scientists at Harvard Med School working on novel methods of controlling systemic inflammation.
I basically agree with all your points regarding the health issues created by our unhealthy American diet which is too high in omega6s and high glycemic index carbohydrates. This is clearly the nations number one health issue and leads not only to atherosclerotic vascular disease and Type2Diabetes, but a whole spectrum of chronic degenerative diseases, allergies and auto immune disorders.
Where I do not agree is on the subject of the importance of DHA vs EPA..EPA due to its structural similarity to arachidonic acid (AA) can act at the same cell and nuclear membrane receptors, the COX and LOX receptors as AA. AA which is derived from omega6s is the most important promoter of chronic systemic inflammation. EPA, but not DHA competes for these membrane receptors with the general action of decreasing over all inflammation. EPA also actively influences t5he PPAR-gamma nuclear membrane receptors which also decreases inflammation.
Because our diets as you point out are so high in n-6s, we need a great deal of EPA. Unfortunately if you try to obtain therapeutic levels of EPA using regular fish oil, you will consume too much DHA which is the portion of fish oil which causes the unpleasant GI effects. You need to either modify your diet or take a more pure form of EPA
respectfully…A.M. Weikel MD
Anthony, I have read the studies by biochemists like William Lands that agree with your comments about Omega-3 and Omega-6 competing for the same receptors. So the implication of that is to increase Omega-3 to overpower the Omega-6.
Doesn’t that however ignore the fact that BOTH Omega-3 and Omega-6 are highly unstable polyunsaturated fats that are subject to oxidation. The solution proposed by the AHA – to consume more Omega-3 to offset our overdose of Omega-6 – therefore subjects us to even more oxidative stress than Omega-6 alone would.
Wouldn’t the much more conservative strategy be to reduce dietary consumption of Omega-6, thereby reducing the need for large doses of Omega-3, and put these two oils into their correct relative balance and at quantities more like the trace requirements the body actually has?
Dear Pone..
You ask, why not just cut down on our n-6 consumption? Well certainly that would do the trick, although you still need EPA. Cutting down on n-6s is not a practical solution for people living in the USA. Our entire food delivery system..ie supermarkets, rely on n-6s. Processed foods have been seed oil dependent since the 1940s. Adding seed oil fraction which is relatively resistant to oxidation, adds flavor and increases shelf life. Prior to the the development of seed oil presses, there were no supermarkets, because food products were too unstable.
There is also another issue besides n-6 consumption which are high glycemic index carbs.
Rapid absorption of sugars causes blood sugar spikes which triggers insulin release. Insulin favors the AA pathway accelerating the rate and percentage conversion of n-6s to AA which increases systemic inflammation. Bottom line, in the USA we need to consume more EPA.
Suggest reading material written by Dr. Bernard Sears..
respectfully A Weikel.
I’ve read Dr. Sears’s books. He certainly makes the case for reducing foods that spike insulin and increasing intake of EPA in controlling AA production. But his protocol seems to give no weight to the beneficial aspects of what he calls the “bad” ecosanoids. Following his protocol, especially his recommendation of 7.5 grams of Omega 3s in extreme cases, would greatly distort the “normal” (optimal?) percentage of n-3s in cell membranes, I assume. Could you comment on this?
Chris, I am all confused. Few months ago there was a report based researched people who consumed high level of omega-3 had high risk of prostate cancer compared to people who consumed high level of omega-6. Please comment on that. Also, can you please advise daily recommended intake of omega 3 and 6 for adult.
This article has an interesting statement that “the ratio of omega-6 to omega-3 matters, but so does the total amount of each.”
Assume that somehow we manage to get our Omega-3 to Omega-6 balance closer to the ideal 1:1 profile. In that case, what is the maximum amount of Omega-6 that we are allowed to ingest, and what is the reason for that limitation?
I live on the coast of australia and eat fish six nights a week not fried in any oil (nonstick pan) . Pizza on the seventh night. No need 4 fish oil.
Non-stick pans contain a cancer causing chemical that transfers slowly over time into your food. You should use cast iron with a splash of canola.
Canola!?!?????
Did you even read the information provided here!?
This is only true for non stick using PFOE and similar. Ceramic coatings and the new diamond like film coatings are non toxic and metal utensil save. They can be found on many stainless steel and cast iron products. Newer research has shown that DLC’s (diamond like compounds) are dense enough to seal the surfaces and prevent leaching of metals from copper and aluminum cookware.
Modern ceramic and DLC nonstick surfaced are not you grannies poison.
HI,
We started our 8 year old on Eye Q (https://www.equazen.com/default.aspx?pid=329) and are on the first month where they say to take 6 caps a day. I’m not sure if this is related, hope you can help, but quite recently, within the last week I’d say (week 3 of the 1st month) – the following is happening and I’d like to know if you think it’s related to the capsules, or just an 8 year old being and 8 year old:
1) Complaining about pain in hands and legs (sound arthritic by how he describes it) – we thought it could be growing pains.
2) Moodiness, anger, and what seems to be some depression.
This has happened quite quickly, usually he’s a great kid – we put him on this stuff to help him with concentration as we found although he’s very bright and one of the top students in his class, he was not able to focus sometimes and get distracted easily, so we thought the product would help that.
In your experience, in just 2-3 week, could this stuff be the cause of his body aches and change in personality?
Thanks
Chris, the Inuit Paradox is that the Western Greenland Eskimo used to eat lots of fat and hardly any vegetables yet they had a very low incidence of cardiovascular disease.
The takeaway in light of recent research on Omega Fatty Acids is to avoid Omega 6 Fatty Acids and get more Omega 3′s & 7′s:
https://www.cardia7.com/omega-6-fatty-acids/
Hi Clare, I’ve read in Dr. Steve ILardi’s book ‘The Depression Cure’ a whole chapter on omega 3 and 6 etc.
Now, he says there is GLA omega 6 (gamma linolenic acid) which is a nice anti-inflammatory – thing is if you’re having lots of EPA from fish etc. it can cut back production of GLA.
So you need something like oatmeal- the slow cook stuff not intant- has lots of it- I think hemp oil too? check this out first though
hope this helps 🙂
Chris et al
We do not consume processed pre packaged foods, nor do we buy supermarket ready meals etc. I cook from scratch. No breakfast cereals, no pasta, no rice, no flours (as in baked foods) are eaten. We are Omnivores, and eat protein of some source with every meal, plus non starchy vegetables, salads etc. Minimal fruit (exception Avo’s and a few berries) is consumed. Therefore we are low in fructose as well.
Dairy is minimal….. goat yoghurt and fresh cream and butter…… in small amounts
I use EV Coconut oil or animal fat to cook with, butter on vegetables. Husband makes his own mayo 50/50 CO/EVO
Question is….. are we deficient in n-6’s?
Both of us are diet controlled T2DM, hence the LCHF approach – it works!
Add chia seed and hemp seed and ground flax seed to my daily 100g yoghurt.
We take a fish oil capsule a day, eat fresh salmon maybe once each week, but still suffer from extreme inflammation. Vascular CVD and vasculitis……
Where are we going wrong? Please don’t tell me to talk this out with my GP…. nutrition is not their modus operandi 🙂
I read all the information I can get hold of about inflammation — PEG -1’s versus PEG-2’s
Help is appreciated.
Hi Clare,
It sounds like you and your husband have a great eatstyle – I don’t like to say diet! I actually eat low(er) carb myself. What are you and your husband’s A1C’s? Do you bake with a lot of almond flour? I’ve read that almond flour is high in Omega-6… Maybe that could be a culprit?
I seem to recall one famous online doctor saying that unless animals are grass fed, the ratio of omega 6 to omega 3 in their will be unfavourably outbalanced. Hence, unless we eat grass fed meat we may be consuming too much omega 6. It’s just a thought you might wish to research.
Hey Chris. I was checking out a video on lecturepad about PUFA intake and SHD risk. He make’s a pretty compelling argument for PUFA consumption as Heart protective. I’d love to get your opinion on this. The lecture should be on the link below. The title of the video lecture is N6 Fatty Acids harmful or helpful if the link doesn’t take you straight there. There’s also some great stuff on lipid metabolism on that site also…Im sure you’ve seen it though 🙂 cheers
https://www.lecturepad.org/index.php/cardiovascular/38-treatment-prevention/1048-n-6-fatty-acids-harmful-or-helpful-n6n3-rations-useful-or-not
*CHD…my bad
Dr. Michael Greger’s lecture from 2003 says everything this article is saying. If you are vegan, and want a vegans point of view, check out his lecture…
Thanks for uploading this video, it contains some excellent information … however, some of his advice seems a little dated. He claims that saturated fats are unhealthy and must be avoided, yet there’s plenty of research to suggest that saturated fats are healthy. They remain stable and don’t oxidise at high temperatures making them excellent fats for cooking.
Dr Greger also advises against salt consumption – but research suggests that salt doesn’t contribute to heart disease, instead it is the ratio of high sodium to low potassium intake that is supposed to cause problems. Potassium is abundant in many fruit and veg.
He also advises against consuming foods containing cholesterol – yet it is now known that the consumption of cholesterol in our food has practically zero effect on our body’s cholesterol levels. The body makes its own cholesterol on a ‘need to’ basis depending on how much inflammation is in the body. Cholesterol, so we’re told, is the ambulance that turns up at the scene of an accident. Cholesterol rectifies the damage caused by inflammation in our arteries, but it gets blamed for causing the problem.
He also cautions against consuming coconut oil – yet we now know this is one of the healthiest oils we can consume.
He also suggests that vegetarians and vegans could get some of their B12 requirements from fortified soy milk, yet we are told by other doctors that soy products – unless fermented – are tremendously detrimental to health, partly because of their phytate and lectin content, along with phytoestrogens which may disrupt hormone balance in some individuals.
He also cautions against eating animal products due to their trans fat content – but there’s research to suggest that trans fats in animal products such as meat and butter do not have a damaging effect on health, to the contrary they have beneficial properties, unlike man made trans fats such as hydrogenated vegetable/seed oils. An interesting article about this can be found on this website:
https://chriskresser.com/can-some-trans-fats-be-healthy
After saying all that, Dr Gregor gives some fascinating information about the dangers of homocystine and how it can be lowered with Vitamin B12, so thanks for uploading the video. I just hope he’s right about it, though. The video is over 10 years old, so perhaps he’s changed his stance on coconut fat etc …